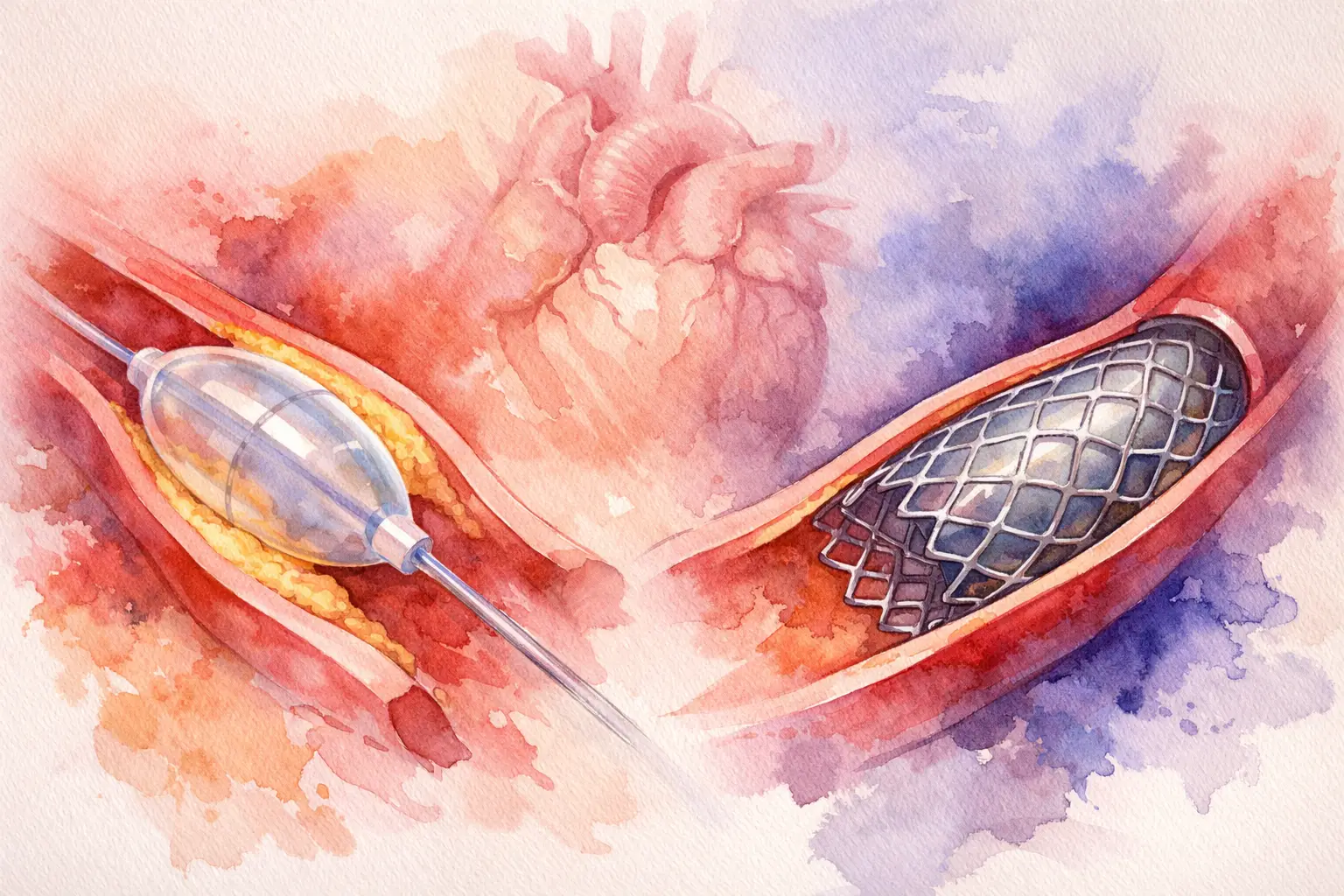
Coronary Balloons vs Coronary Stents
A cath lab rarely asks a simple question when planning inventory. The real issue behind coronary balloons vs coronary stents is not which device is better in isolation, but which device fits the lesion set, operator strategy, and stocking model of the facility. For procurement teams, that distinction matters because balloons and stents serve overlapping but not interchangeable roles across PCI workflows.
Hospitals and distributors that buy only by broad category can run into avoidable gaps. A lab may have adequate DES coverage but limited semi-compliant balloon options, or a strong balloon assortment but insufficient stent diameters and lengths for routine coronary work. In practice, procedure success depends on having the right mix of both.
Coronary balloons vs coronary stents in clinical use
Coronary balloons are catheter-based devices used to dilate stenotic coronary lesions. In PCI, they may be used for lesion crossing, predilation, postdilation, and in some cases definitive treatment, depending on lesion morphology and physician intent. The category includes semi-compliant balloons, non-compliant balloons, specialty balloons, and drug-coated balloons in selected settings.
Coronary stents are scaffold implants deployed within the vessel to maintain luminal patency after lesion preparation. In modern coronary intervention, drug-eluting stents remain a standard treatment option for many de novo lesions because they provide mechanical support and reduce restenosis risk compared with balloon angioplasty alone. Bare-metal stents still exist in some markets, but DES dominates routine coronary use.
The practical point for buyers is straightforward. Balloons are procedural enablers across almost every PCI case. Stents are often the definitive implant, but not every balloon case ends with a stent, and no stent case succeeds without the right balloon support strategy before or after deployment.
Why the comparison is often misleading
Procurement discussions sometimes frame balloons and stents as alternatives in a one-line comparison. That oversimplifies actual device demand. In most coronary workflows, balloons and stents are sequential tools, not direct substitutes.
A semi-compliant balloon may be selected for initial predilation because it tracks well and conforms to vessel anatomy. A non-compliant balloon may then be used for lesion optimization or high-pressure postdilation. The stent, if implanted, addresses recoil or dissection risk and creates durable scaffolding. If the lesion is in-stent restenosis or a small vessel under a specific treatment strategy, a drug-coated balloon may be considered instead of placing another metal layer. So the answer is often not balloons or stents, but which balloon types plus which stent platforms should be available.
For sourcing teams, this means utilization patterns should be reviewed together. Ordering stents without adequate lesion preparation inventory creates procedural inefficiency. Ordering balloons without enough implant depth can force substitutions that clinicians may not prefer.
Where coronary balloons have the advantage
Balloon-based treatment has clear value in several scenarios. First, balloons are essential for lesion preparation. Calcified, tight, tortuous, or resistant lesions often require staged preparation before a stent can be delivered and expanded properly. Even in standard lesions, operators routinely depend on predilation or postdilation balloons to optimize the result.
Second, balloons avoid leaving a permanent implant when the treatment plan supports that approach. This can matter in selected in-stent restenosis cases, small vessels, bifurcation strategies, or anatomy where adding another stent layer is less attractive. Drug-coated balloons are especially relevant in those discussions, although adoption varies by market, indication, and physician preference.
Third, balloons offer breadth within a relatively compact inventory structure. A lab can stock multiple diameters, lengths, compliance profiles, and specialty configurations to support a wide lesion mix. The unit economics and storage approach differ from implantable devices, which can make balloon assortment planning more flexible.
That said, balloons alone do not solve recoil, major dissection, or the need for durable vessel scaffolding. Their advantage is precision and versatility, not universal final treatment.
Where coronary stents have the advantage
Stents remain central because they address a problem balloons cannot always control after vessel expansion. When plaque burden, vessel recoil, or dissection threatens lumen durability, a coronary stent provides structural support that balloon angioplasty alone does not. This is a major reason DES became standard across many coronary lesion subsets.
Stents also offer predictability in routine de novo coronary disease. For many operators, a contemporary DES platform with known deliverability, radial strength, and drug-release characteristics is the expected endpoint once the lesion is prepared. Procurement teams generally see this reflected in stable demand for major branded stent families from established manufacturers.
Another advantage is protocol familiarity. Many centers have strong internal experience with specific stent platforms, including known sizing behavior, crossing profile, and postdilation expectations. That familiarity reduces variation and supports procedural consistency. Buyers should not underestimate this factor when evaluating equivalent-looking alternatives across brands.
The trade-off is that stents are permanent implants. They introduce considerations around metal layers, future reintervention strategy, vessel anatomy, and antiplatelet management. They also require careful SKU planning across diameters and lengths to avoid stockouts in core sizes while limiting slow-moving inventory.
Procurement factors behind coronary balloons vs coronary stents
From a purchasing standpoint, the category decision is less about preference and more about case mix, physician practice, and inventory continuity. A center with high routine PCI volume may need broad DES coverage combined with strong demand for semi-compliant and non-compliant balloons. A center handling more complex lesions may place greater emphasis on specialty balloons and high-pressure postdilation options. A distributor serving multiple hospital profiles may need depth across both categories rather than concentration in one.
Brand standardization matters. Clinicians often request exact manufacturers because crossing performance, shaft behavior, compliance characteristics, and deployment feel are not interchangeable in practice. Recognized coronary platforms from companies such as Abbott, Boston Scientific, Medtronic, Cordis, Terumo, and Asahi tend to anchor purchasing decisions because physicians already know how these products perform in the lab.
Shelf management also differs. Balloon inventory often turns through a wider set of routine procedural uses. Stent inventory may be higher in value and more sensitive to gaps in key diameters and lengths. Buyers should review actual consumption by lesion type, not just by annual category spend.
International procurement adds another layer. Export buyers often need consolidated sourcing across several branded coronary lines rather than a single-category supplier. That is one reason some procurement teams work with wholesale partners such as IMTMedicalDevices.com when they need recognized manufacturers, quote-based volume purchasing, and cross-border supply coordination from one source.
Stocking logic for cath labs and distributors
A practical stocking model usually starts with the procedural pathway rather than the catalog tree. If most coronary cases begin with workhorse lesion preparation, then core balloon SKUs need to be protected first. If the center has standardized on a few DES families, then those stent diameters and lengths should be maintained with enough depth to cover routine and urgent demand.
It also helps to separate fast movers from strategic coverage items. Common balloon diameters and lengths may require high availability because they support both predilation and postdilation. Core stent sizes may need deeper stock than edge-case lengths that move slowly. This is where historical usage data becomes more useful than generic market assumptions.
For distributors, the challenge is broader. The goal is not only to carry coronary balloons and coronary stents, but to align manufacturer mix with local physician preference and reimbursement realities. A broad portfolio has value only if the right SKUs are available when a customer asks for an exact product reference.
Choosing between category depth and brand breadth
There is no single ideal ratio of balloon inventory to stent inventory. It depends on how coronary volume is distributed across routine PCI, complex PCI, restenosis management, and physician-specific technique. Some labs benefit more from deeper balloon specialization. Others gain more from maintaining broader stent platform access.
What usually performs best is disciplined category coverage with selective brand breadth. Too little variety creates procedural workarounds. Too much variety can fragment purchasing and slow turnover. The strongest procurement approach is to identify the branded platforms clinicians actually use, maintain continuity in the core range, and fill secondary needs with deliberate rather than reactive buying.
For professional buyers, coronary balloons vs coronary stents is best treated as a planning question, not a debate. Balloons shape access, preparation, and optimization. Stents deliver scaffolding where the vessel needs it. The value is in sourcing both categories with enough precision that the physician does not have to compromise at the table.