Asahi Fielder Guidewire Review for Buyers
A Fielder request usually shows up when the case plan includes ambiguous proximal caps, small channels, or a need to probe without committing to high tip load early. If you are buying for a cath lab or stocking for resale, the decision is less about hype and more about repeatable use cases, sizing, and how reliably the wire behaves when different operators pick it up.
This review Asahi Fielder guidewire overview is written from a procurement angle: what you are really paying for, where it fits in a typical coronary CTO wire escalation strategy, and what to clarify before you place a quote request.
Review Asahi Fielder guidewire: where it fits clinically
Asahi Intecc’s Fielder family is typically positioned as a workhorse for soft, trackable crossing attempts - especially when the intent is to explore microchannels or move through tortuosity with a lower risk of aggressive vessel injury compared with higher-gram, penetrative CTO wires. Buyers generally see it requested in coronary programs that do consistent CTO volume or complex coronary work and want predictable early-step options on the shelf.
From an inventory standpoint, the Fielder line tends to be requested alongside microcatheters and support catheters because performance is highly dependent on how the wire is delivered and supported. If your clinicians routinely pair it with a specific microcatheter brand, keep that pairing consistent in your stocking plan to reduce “wire blamed for support” situations.
Fielder variants and what procurement should confirm
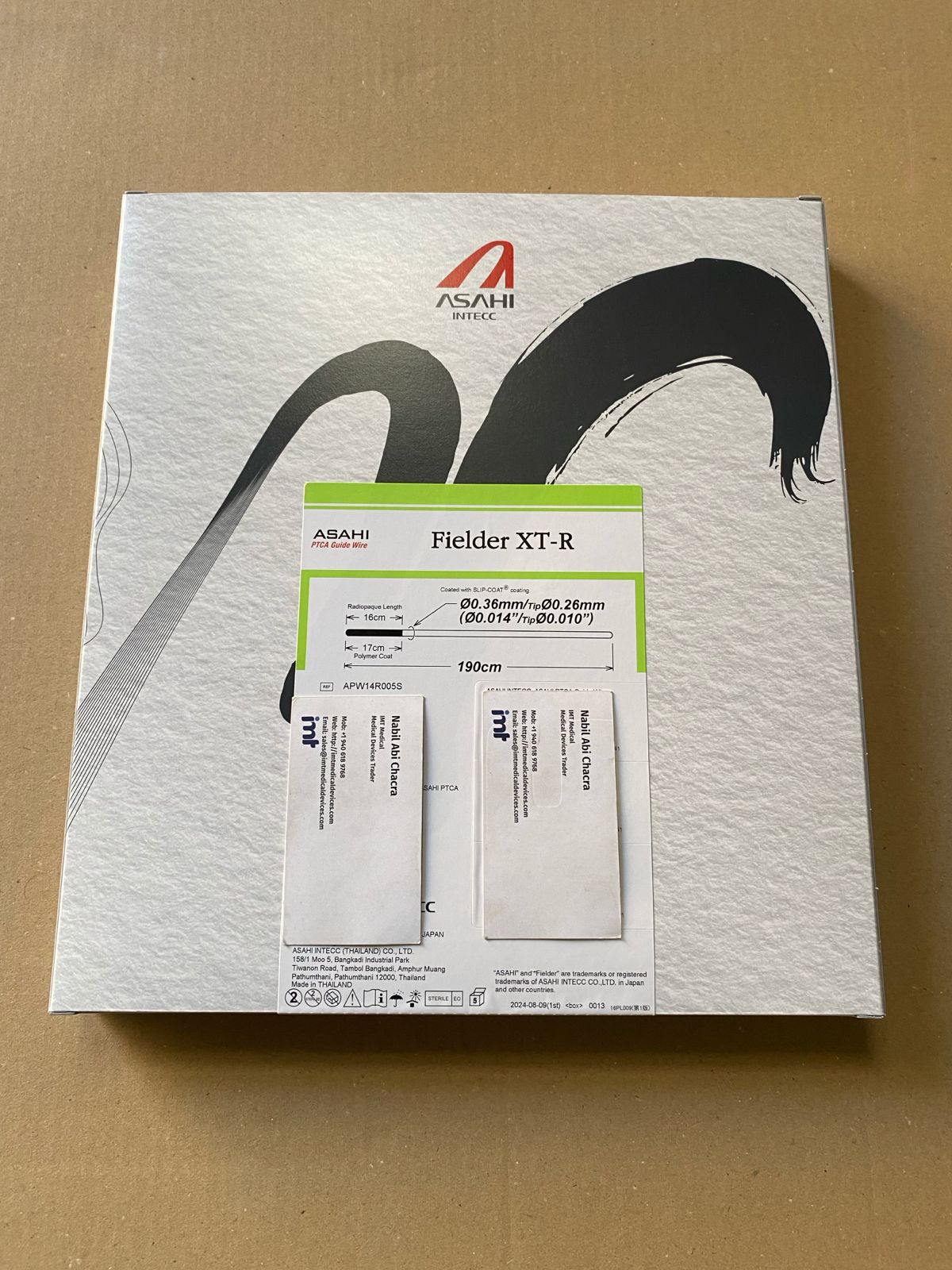
Most purchasing friction around the Fielder family happens when “Fielder” is used as shorthand. Operators often mean a specific variant. If you are buying for a hospital that rotates staff or you supply multiple accounts, confirm the exact Fielder model name on the request and match it to the manufacturer reference/ordering code used in their preference card.
In practical terms, the variants are selected for slightly different behaviors: how the tip feels when probing, how the coating behaves in tight anatomy, and how much tactile feedback is preserved. That means substitution risk is real. If you quote the wrong Fielder version, the product may still be clinically usable, but the operator may treat it as a different step in escalation - and your “equivalent” swap becomes an avoidable complaint.
If you are consolidating SKUs, the cleanest approach is to stock the variant(s) that your physicians actually name, then only add adjacent variants when you can tie them to a specific use pattern or physician preference.
Handling and deliverability: what users tend to value
The most consistent positive feedback around Fielder wires is deliverability - the sense that the wire advances without feeling sticky, and that it navigates tortuosity with less tendency to buckle compared with less refined, generic hydrophilic offerings. In complex coronary anatomy, that “clean travel” matters because it reduces time spent repositioning or re-shaping the tip.
Another practical advantage is that the Fielder family is often used to feel out the path before committing to a more penetrative wire. In cath labs that run a disciplined escalation strategy, this makes the Fielder a repeat-use item. For procurement, repeat-use items are where you want predictable supply and consistent lot-to-lot performance, because small changes in coating feel become noticeable when the product is used weekly.
Trade-off: very slippery hydrophilic behavior can reduce tactile feedback for some operators, especially when the intention is to “read” the cap or detect subintimal entry early. If your physicians emphasize tactile feel, they may request a specific Fielder variant or may move earlier to a different Asahi CTO wire depending on technique. The key is not to assume that “hydrophilic = always better.” It depends on operator style, microcatheter support, and lesion morphology.
Lesion selection: when the Fielder can be the right first step
From a stocking standpoint, the Fielder is easiest to justify when your accounts do any of the following with frequency: CTO exploration in softer caps, cases where channel tracking is attempted, or complex non-CTO lesions where a slippery, trackable wire reduces friction during device delivery.
It is less defensible as a universal default wire for every case, because many labs already standardize on other workhorse coronary wires for routine PCI and reserve the Fielder for specific moments in escalation. That affects par levels. If your lab does limited CTO volume, buying deep on Fielder SKUs can create slow-moving inventory.
Also consider that some operators treat a Fielder as a “test and exit” wire: they probe briefly, then either advance successfully or switch quickly. That can produce higher unit consumption than you would expect from procedure volume alone, because one case can burn multiple wires when the anatomy is challenging.
Compatibility and support: why microcatheter pairing matters
A Fielder wire’s behavior is not isolated. In real purchasing terms, the “system” matters: guiding catheter support, microcatheter selection, and the lab’s standard torque device.
If your accounts standardize on microcatheters for CTO work, confirm that they have enough microcatheter inventory to actually leverage Fielder performance. A lab that is short on microcatheters may report poor crossing or poor steerability, when the constraint is support rather than wire quality.
From a distributor perspective, bundling quoting - wire plus the microcatheter brands your accounts use - reduces back-and-forth and makes procurement simpler. It also reduces last-minute substitutions that can create clinician pushback.
Sizes, lengths, and what to confirm before quoting
Hospitals and distributors often lose time on basic spec confirmation. Before quoting any Asahi Fielder guidewire, validate the requested length and any packaging/unit-of-measure expectations in the account’s purchasing system.
Length selection is usually driven by lab standard operating practice and the type of procedures they do most. If an account routinely runs complex CTO cases with microcatheters and long device exchanges, they may prefer a consistent length across their CTO wire set to reduce variability. If they do mixed coronary work with occasional CTO, they may keep fewer length options and accept substitutions only within a narrow range.
Also confirm whether the request is for a single wire or a box quantity. Some accounts enter “1” meaning “1 box,” others mean “1 unit.” If you supply across Gulf countries, Latin America, or Asia, this unit-of-measure mismatch is one of the most common sources of delays at customs clearance or during receiving.
Supply-chain realities: lead time, shelf life, and substitution risk
Asahi wires are branded, preference-driven devices. When an operator writes a specific wire into a CTO algorithm, the lab will often resist substitution. That makes availability more important than small price deltas.
If you are stocking for a hospital that avoids local distributors, the value is consistency: same manufacturer, correct model, and stable replenishment. Confirm lot dating and shelf life before shipment, especially if the account buys in larger quantities to reduce emergency orders.
If a substitution is unavoidable, treat it like a controlled change. Provide the exact alternative model name and confirm clinical acceptance before shipping. For distributors reselling into competitive markets, this reduces returns and reduces disputes with end users.
Buyer checklist: what to ask for a clean purchase order
To reduce friction between the cath lab request, the purchasing department, and your own fulfillment team, the fastest path is to lock down the identifiers and shipping requirements up front. At minimum, you want the exact Asahi Fielder variant name, the wire length, the target quantity (unit vs box), and any country-specific documentation needs.
If the account requires serialized tracking, special labeling, or specific incoterms, confirm those before you issue a pro forma invoice. These details matter more for wires than many people expect because wire orders are often placed urgently, and urgent orders are where paperwork mistakes are most expensive.
For buyers who need a dependable source of branded interventional inventory across coronary, peripheral, and neurovascular categories, IMTmedicaldevices.com is typically used as a quote-driven channel - you submit the exact product request and receive availability and shipment terms aligned to your destination.
When the Fielder is a good buy - and when it is not
The Asahi Fielder family is a strong buy when your users specifically request it for CTO exploration or channel tracking, and when your lab has the microcatheter and support setup to use it as intended. It is also a practical stocking choice for distributors supplying multiple accounts where Asahi is a standard brand in the region.
It is a weaker buy when the account has low CTO volume, no consistent technique requiring it, or a history of frequent “any equivalent” substitutions. In those environments, the Fielder can become slow-moving inventory or a product that gets blamed for system-level limitations.
A helpful closing thought: when you treat a Fielder request like a SKU-identification problem instead of a generic “CTO wire” order, you eliminate most procurement delays - and you protect clinician confidence in the inventory they reach for under pressure.