Cath Lab Buying: Disposable Procurement Checklist
A case gets delayed for one reason more often than most teams admit: the disposable is technically “in stock,” but it is the wrong size, the wrong shaft length, the wrong tip configuration, or the wrong compatibility for the planned device. In interventional cardiology, that is not a paperwork problem - it is a procurement specification problem.
This practical procurement checklist interventional cardiology disposables is written for buyers who already know the brands and categories, but want fewer surprises at receiving, fewer last-minute substitutions, and fewer urgent emails from the cath lab.
Start with the order unit: procedure kit vs SKU-level build
Some hospitals prefer procedure kits (radial kit, diagnostic coronary kit, PCI starter kit). Others buy SKU-by-SKU. Either can work, but the risk profile is different.
Kits reduce line items and speed purchasing, but they also hide variability. If one component changes (needle gauge, introducer length, hemostasis valve style), the kit may still ship “correctly” while the lab experiences a workflow change. SKU-level builds take more time upfront, but they let you lock exact part numbers and qualify alternates deliberately.
If your facility has frequent physician preference changes or multiple operators with different techniques, SKU-level control usually produces fewer day-of-case issues.
Define your “no-substitution” list
Not every disposable needs a hard lock. Guidewires, balloon catheters, and stents are usually preference-sensitive. Basic syringes and bowls usually are not. Your goal is to identify the items that cannot be swapped without clinical or workflow impact.
A practical way to set this is by category. Many teams treat these as no-substitution unless a physician signs off: coronary guidewires (workhorse and specialty), guiding catheters (curve and French size), balloon catheters (diameter, length, compliance class), drug-coated balloons (brand specific), coronary stents (platform specific), aspiration thrombectomy catheters (ID and length), and vascular closure devices.
For everything else, define an acceptable alternate list and document it in the item master so urgent purchasing does not create new, undocumented standards.
Build the checklist around three use cases
Interventional cardiology disposables are not one shopping list. The same product category is bought differently depending on whether you are supporting diagnostic angiography, PCI, or adjunct peripheral work.
Diagnostic coronary (baseline stock)
Diagnostic cases consume high volume, and the goal is repeatability. Make sure your checklist captures the exact combinations the lab actually uses: sheath size and length (radial vs femoral), diagnostic catheter curves, manifolds, torque devices, hemostasis valves, and contrast delivery accessories.
The key procurement detail is compatibility. A 5F workflow needs 5F-compatible valves and catheters, and your standard must match imaging, injectors, and typical access strategy.
PCI (preference and escalation stock)
PCI adds the preference-sensitive items. Here, the checklist needs to go beyond “balloon catheter” and “guidewire.” You need a controlled set across diameters, lengths, and performance tiers.
For balloon catheters, your item master should differentiate: pre-dilation vs post-dilation, semi-compliant vs non-compliant, rapid exchange vs over-the-wire (if relevant), and shaft length. For guidewires, capture both workhorse and specialty (polymer-jacketed, tapered tip) with the exact tip load and coating style the physicians expect.
Escalation stock matters as much as core stock. If you only buy the common sizes, the team will borrow from other rooms, open “just in case” items, or request emergency purchases. That raises cost per case and increases expiry risk.
Complication management and bailout
Bailout disposables can be low turnover, but they cannot be missing. Your checklist should include aspiration options, covered stents if used, pericardiocentesis-related items (as applicable), and closure alternatives for access complications.
This is where procurement needs a realistic par level strategy: keep minimal but sufficient quantity, rotate stock across sites if you operate multiple labs, and watch expiration dates monthly.
Map each category to the exact identifiers procurement needs
A procurement checklist that only lists categories still fails at receiving. The checklist should force identification at the SKU level where it matters.
For each disposable line item, capture:
- Manufacturer (for example: Medtronic, Boston Scientific, Abbott, Terumo, Cordis, BD, B. Braun, Ethicon)
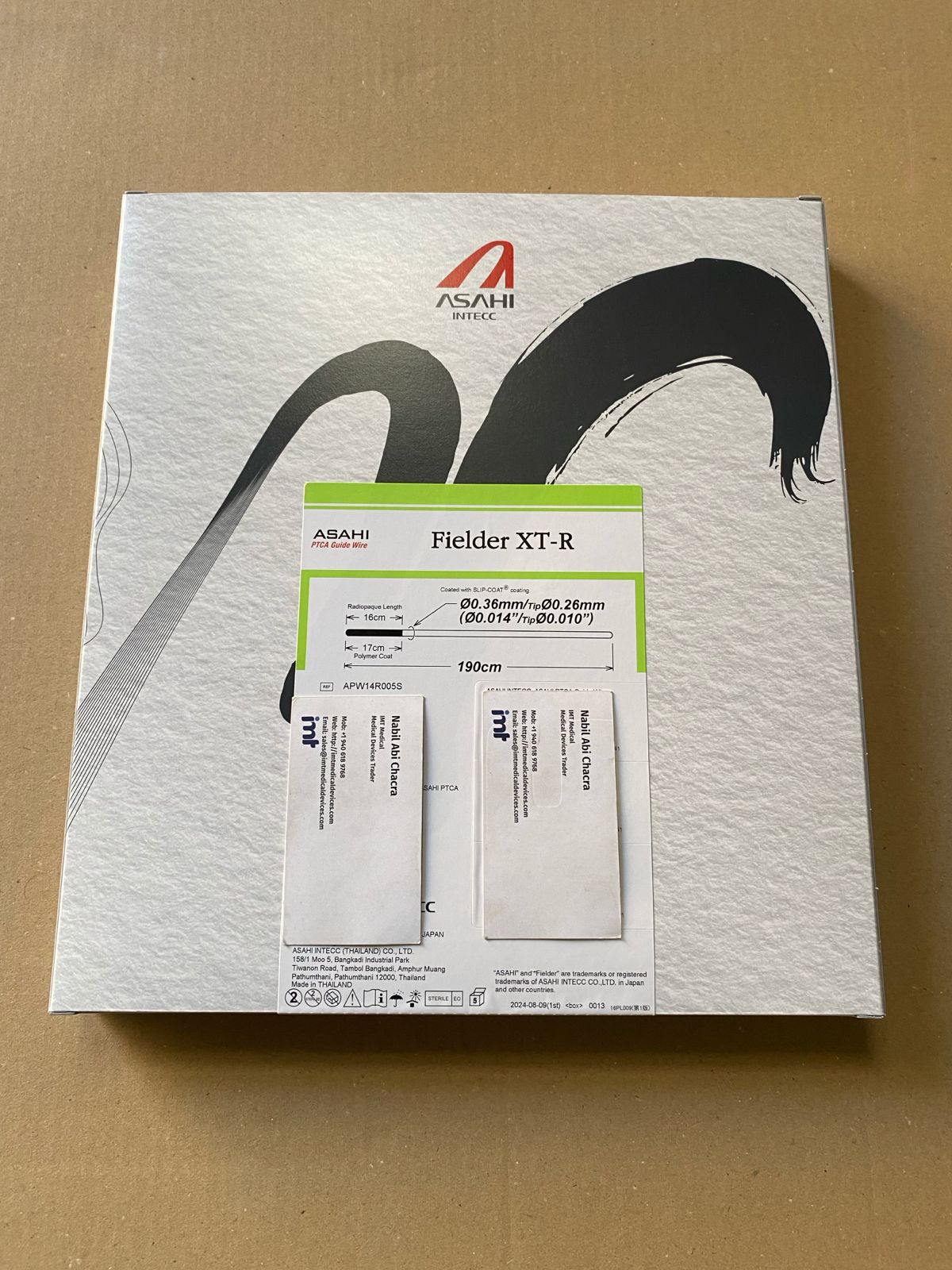
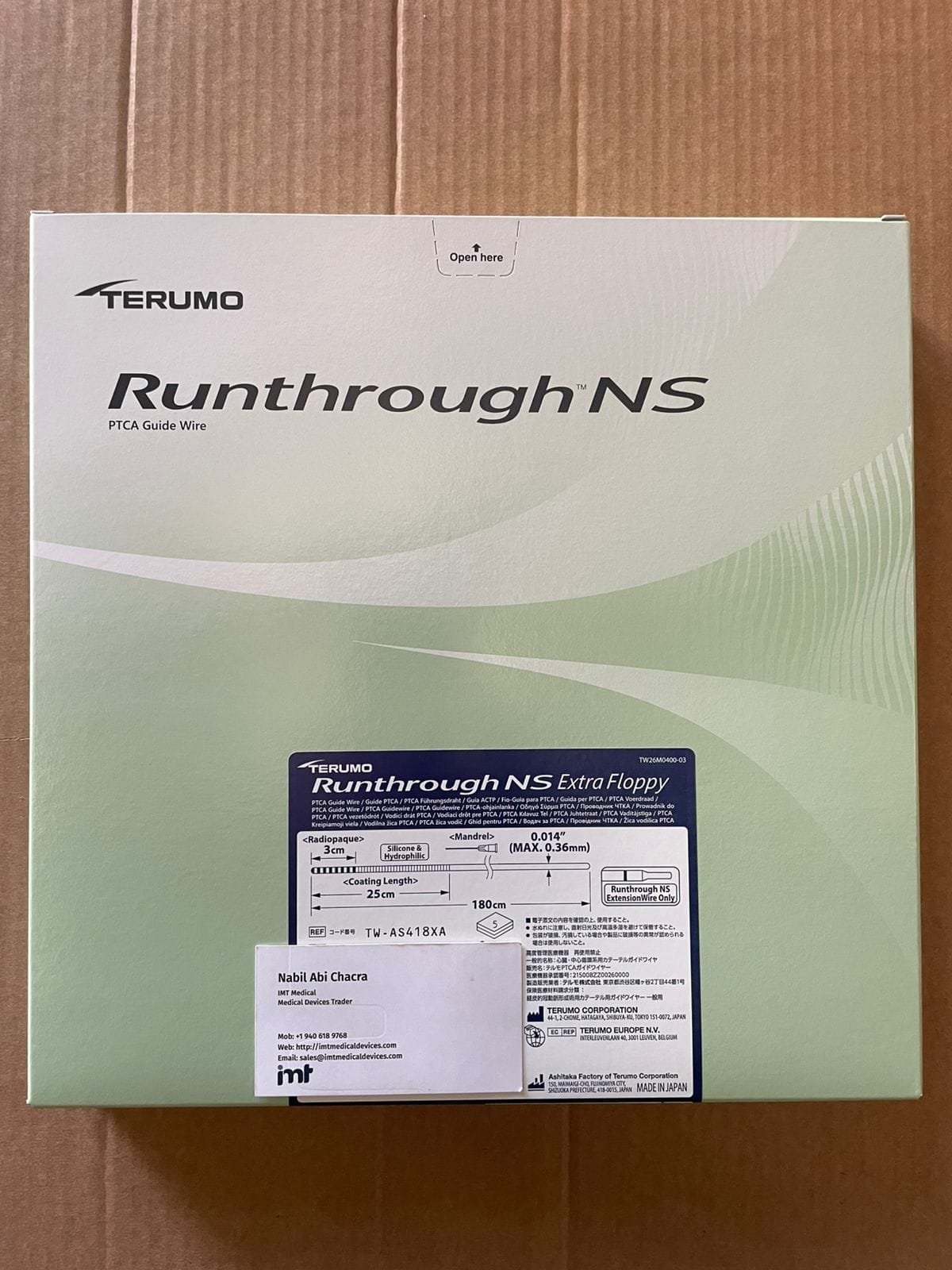
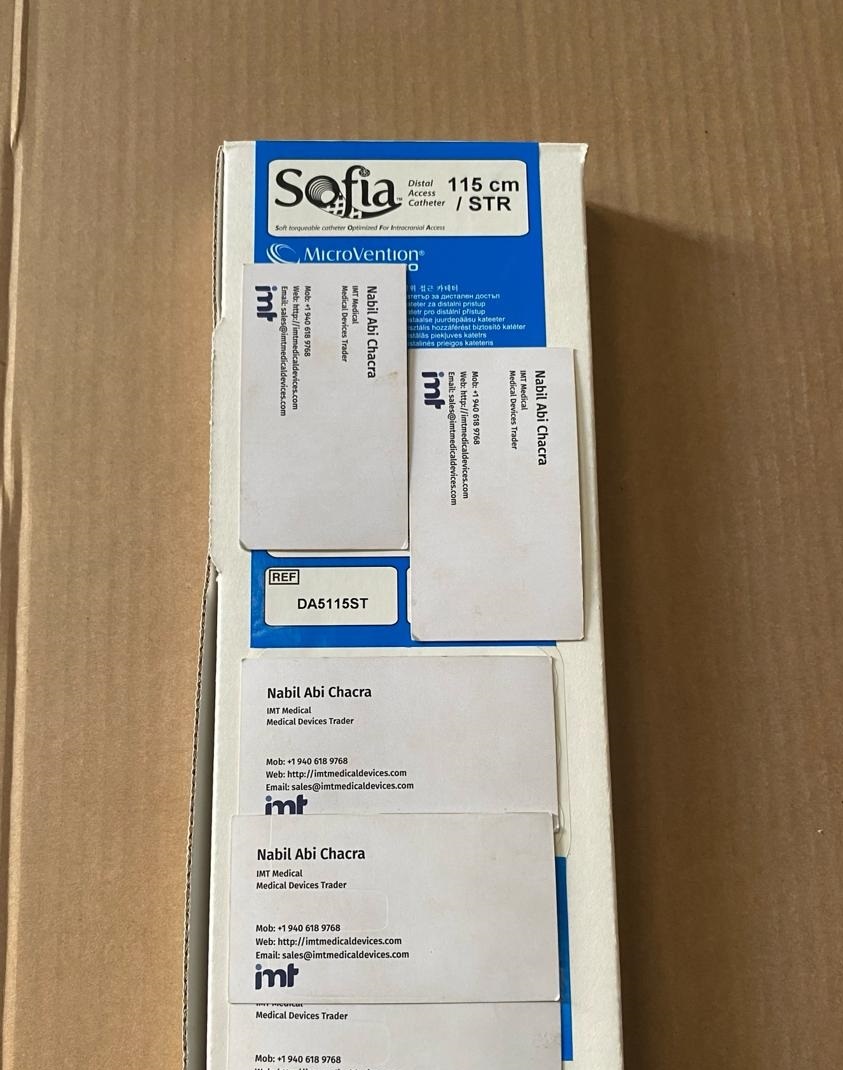
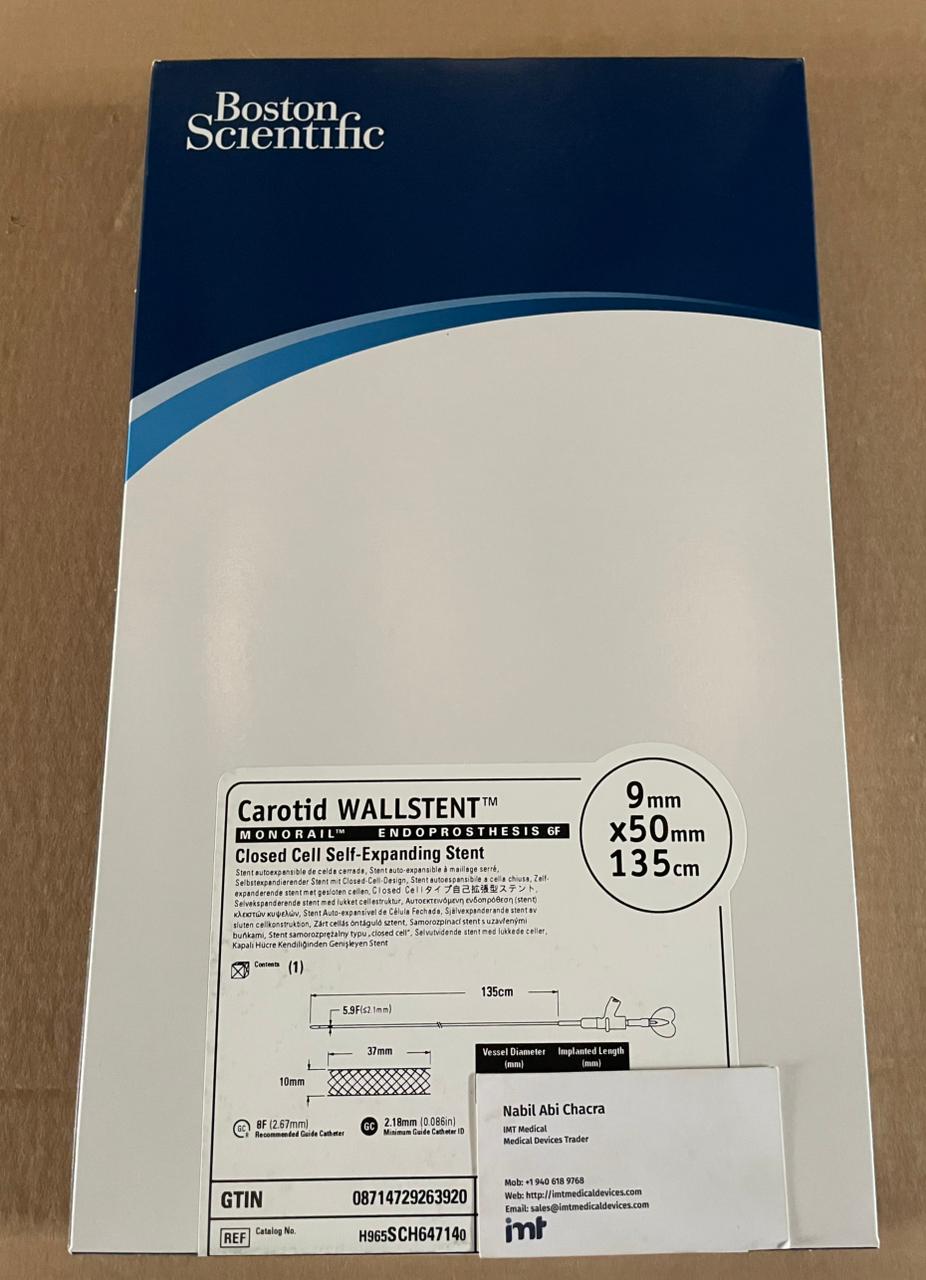
- Product family name (as printed on the box)
- Exact part number or catalog number
- Key attributes: French size, working length, tip shape/curve, wire diameter and length, balloon diameter and length, stent diameter and length, compatibility notes
- Sterility and packaging (single vs double pouch, box count)
- Shelf life/expiry and any temperature constraints
If you operate across borders (common in the Gulf, Latin America, and parts of Asia), add the regulatory or import identifiers you routinely need: country-specific labeling, lot traceability format, and any required certificates requested by your receiving department.
Control substitutions with a tiered alternate policy
Substitution happens. The question is whether it is controlled.
A workable policy is tiered:
Tier 1: Exact SKU only. No substitution without written physician approval.
Tier 2: Same manufacturer, same product family, alternate size within a defined range (for example, balloon length change but same diameter and compliance class).
Tier 3: Cross-manufacturer equivalent allowed from a pre-approved list.
This approach prevents “closest match” decisions by someone who is trying to help but does not live in the cath lab. It also makes vendor conversations faster because you can request quotes that match your tier rules instead of negotiating during a shortage.
Set par levels by consumption, not by feeling
Par levels should be grounded in case mix and lead time.
If you have predictable diagnostic volume but variable PCI complexity, your par levels should look different by category. Diagnostic catheters and sheaths might be stocked deeper because they turn fast. Specialty wires and niche balloon sizes might be stocked shallower but must exist in the building.
Lead time changes the math. When you are purchasing internationally or bypassing a local distributor, you may accept a longer replenishment window in exchange for access to exact branded inventory. That is workable if you set reorder points based on real transit time plus customs/receiving time, not just supplier ship time.
Receiving checklist: verify what the cath lab will notice
Most procurement errors are discovered only after the box is opened in the procedure room. Tighten receiving so you catch the issues earlier.
At receiving, verify part number, quantity per box, and expiration date against the PO. For preference-sensitive disposables, add a second verification step: confirm the key attributes printed on the label match the intended use (size, length, curve). This takes minutes and prevents the “we have it, but not that one” scenario.
Lot and serial capture should match your hospital’s traceability requirements. If your cath lab logs implantables by lot, make sure your receiving workflow preserves lot integrity and does not mix partial boxes without documentation.
Expiry and slow-mover strategy (what you do with the long tail)
Interventional cardiology inventory has a long tail of low-use SKUs that still need to exist. This is where cost control is won or lost.
If you see repeat expirations in a specific diameter or length, adjust the standard set. Either remove it, reduce quantity, or replace it with a neighboring size that the physicians accept. If the item is clinically necessary but rarely used, consider a minimal on-hand quantity with a documented rapid replenishment plan.
Stock rotation across multiple sites is often the cleanest fix when you have more than one cath lab or satellite facility.
Quote requests that actually get you the right product
Suppliers can only quote accurately when the request is precise. When requesting pricing, include the manufacturer, exact part number, and the attributes that matter. If you are willing to accept alternates, state your tier policy in the request so the quote comes back structured, not as a list of “similar” items.
If you need branded interventional inventory across coronary, peripheral, and neurovascular categories, keep your sourcing consolidated where possible so your item master stays consistent across product families. Teams that buy from too many channels often end up with duplicated SKUs that look similar but behave differently in the lab.
For buyers who want a catalog-first way to source branded disposables by manufacturer and part number, IMTmedicaldevices.com is typically used as a fast path to identify items and initiate quotes without rewriting specifications.
The checklist mindset that prevents case-day surprises
Treat disposables like engineered components, not generic supplies. When you force every line item to carry a manufacturer, part number, and the one or two attributes the physician will actually notice, your procurement process stops being reactive.
The most helpful habit is simple: when the cath lab says, “We need a guide catheter,” ask, “Which curve, which French size, which working length, and what is the exact catalog number you want on the shelf?” That one question, repeated consistently, eliminates most of the friction between purchasing and the procedure room - and keeps the schedule moving.