How to Source Medical Device SKUs Fast
If you have ever had a case delayed because the shelf had the right product category but the wrong exact part number, you already know what “SKU sourcing” really means in interventional care. It is not finding “a coronary wire.” It is finding the exact wire a physician expects, in the correct tip load, coating, length, and packaging configuration - and getting it delivered inside the window your schedule can tolerate.
This is a practical workflow for how to source medical device skus in high-acuity cardiovascular, peripheral, and neurovascular programs. It is written for people who buy by part number, manage standardization, and have to explain substitutions when they happen.
Start with the SKU, not the category
For interventional disposables, category-first sourcing is where errors start. A “balloon catheter” search can return dozens of options that are clinically non-interchangeable. The cleanest process is to begin with the manufacturer SKU (or catalog number) and then validate that SKU against procedure need.
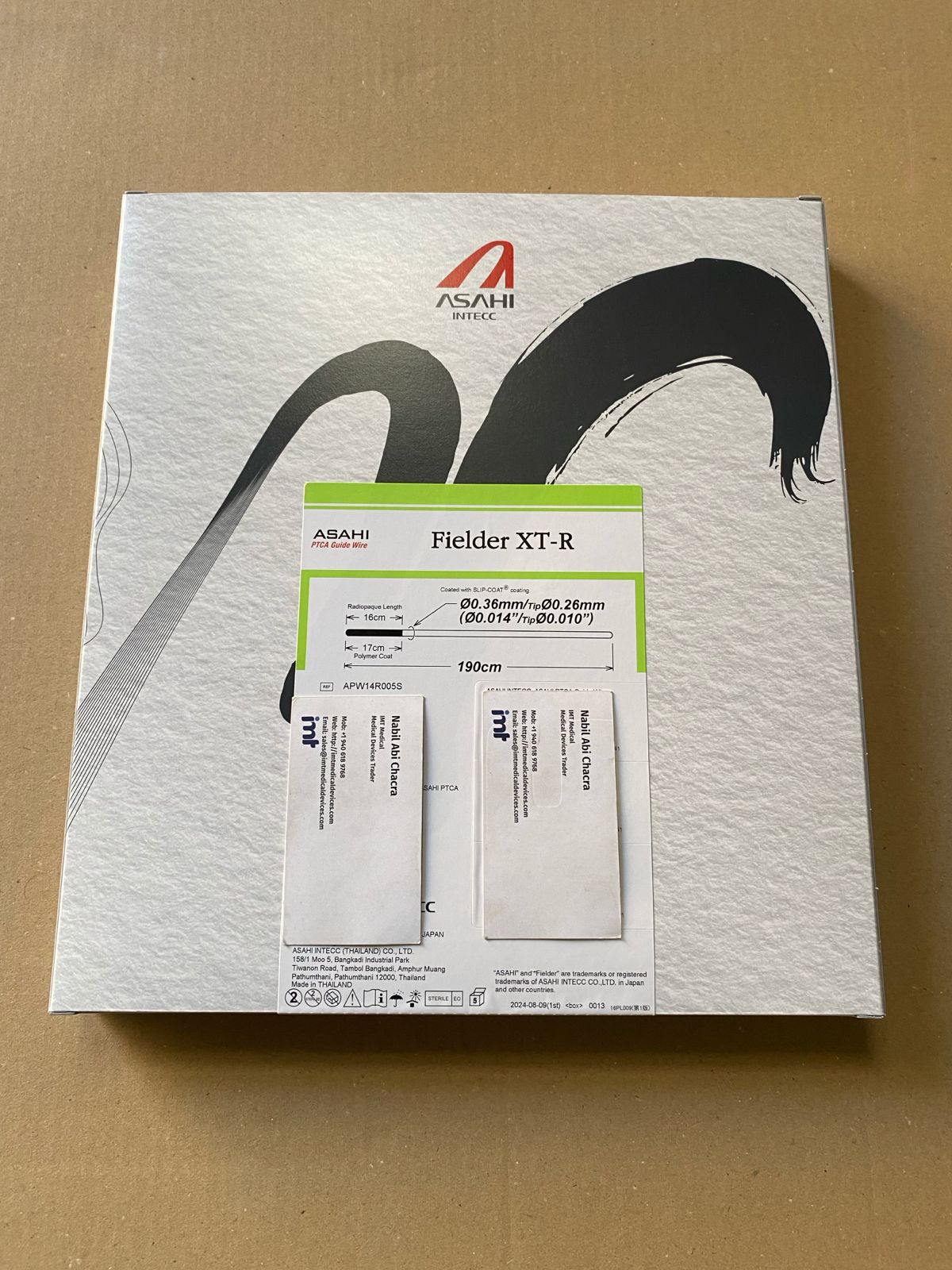
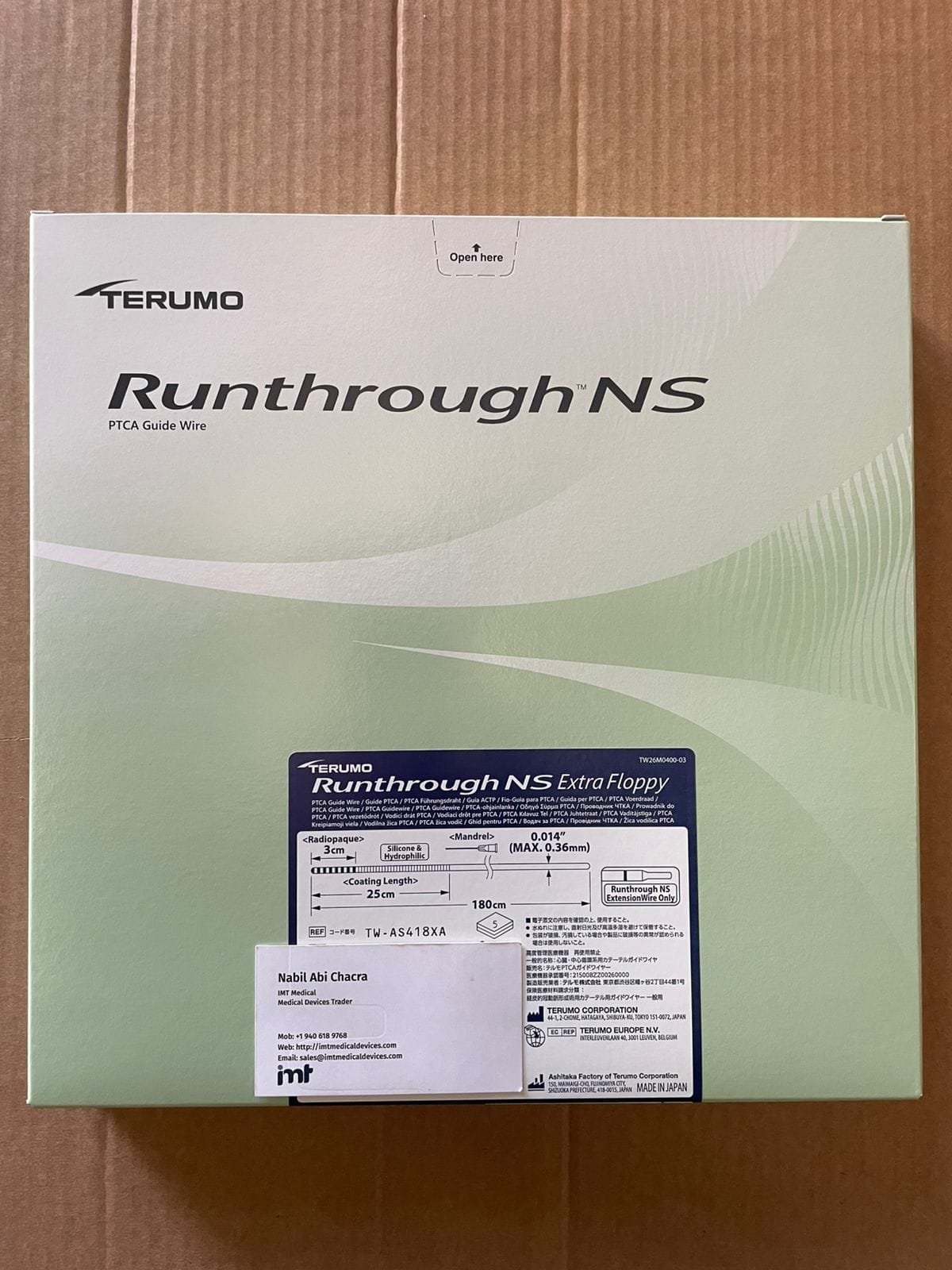
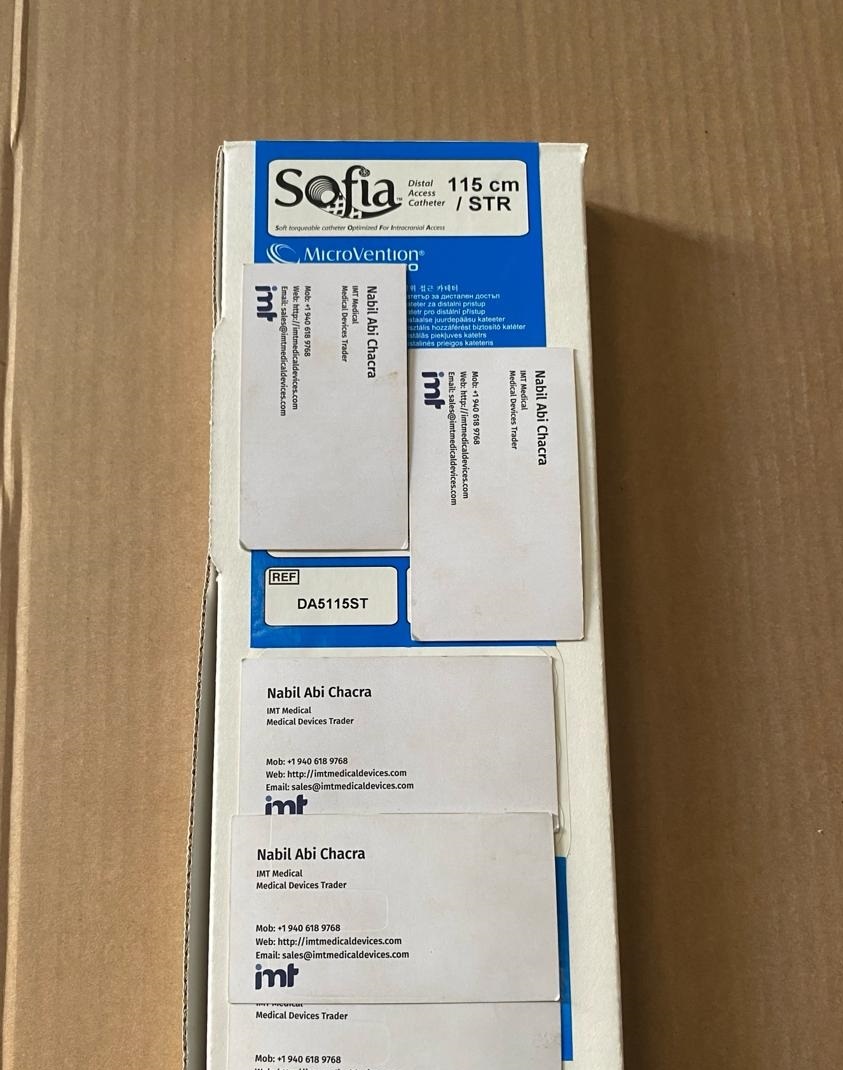
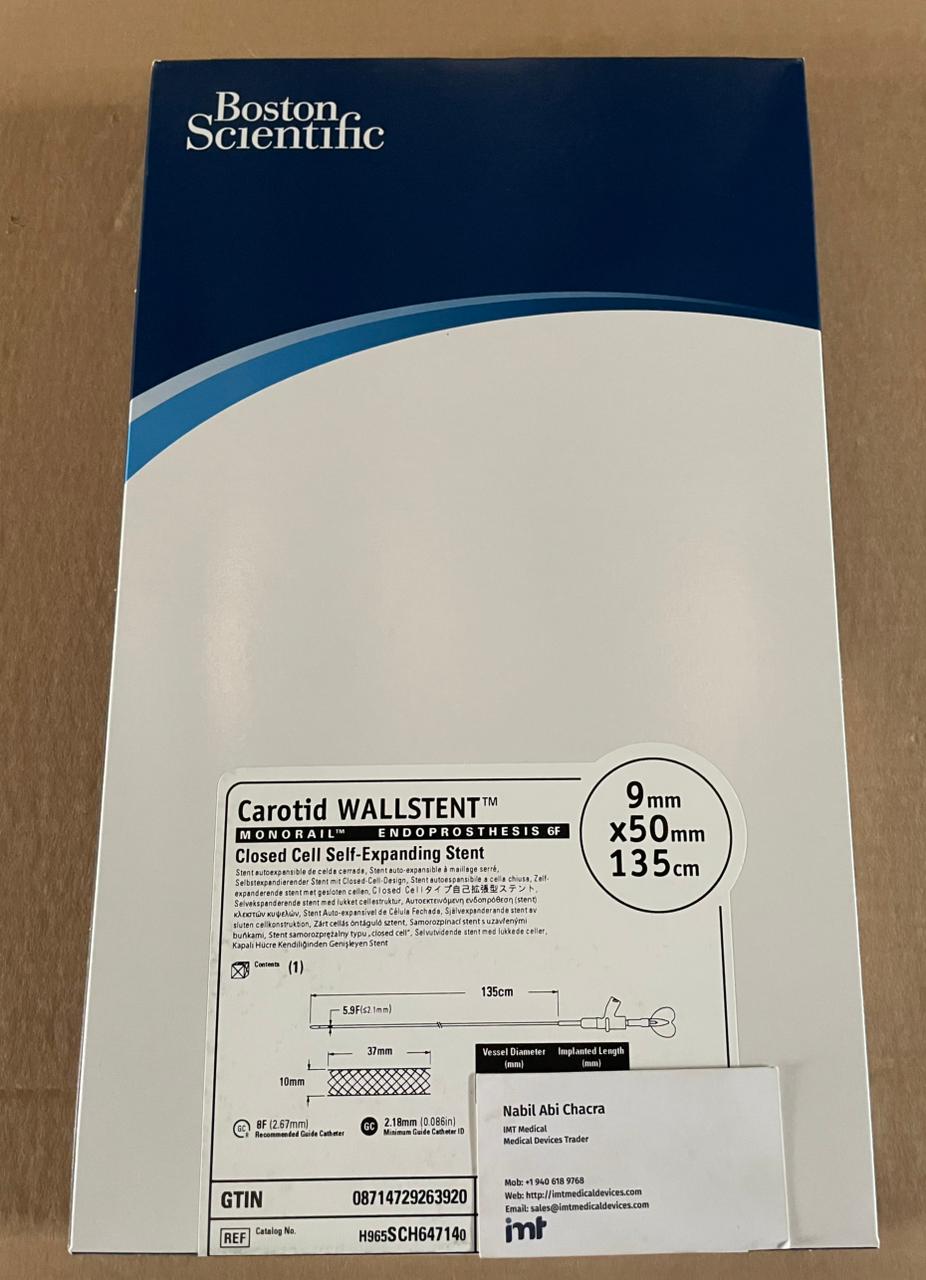
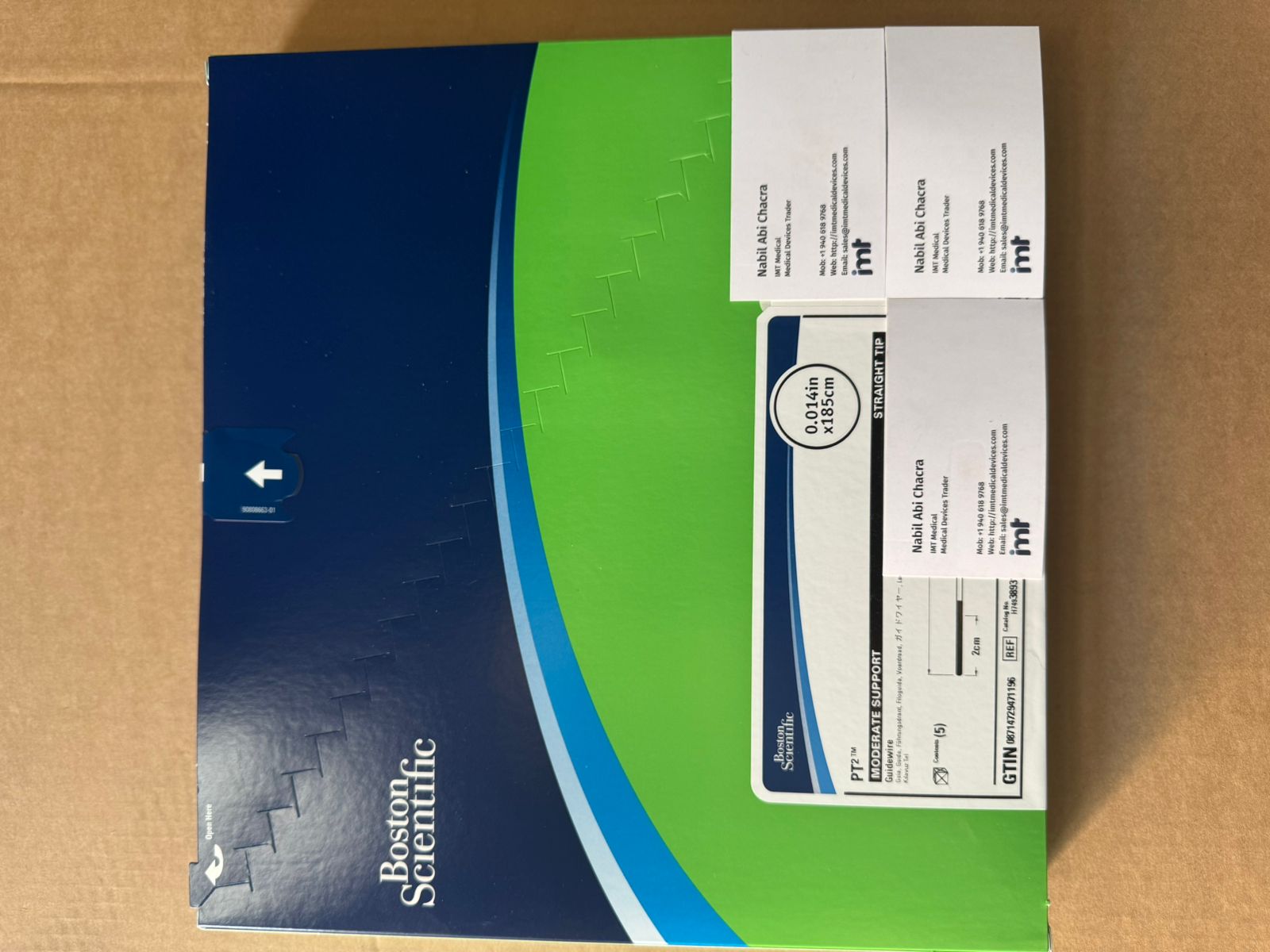
If the request comes from a physician preference card, a past PO, or a case cart pick list, pull the identifier exactly as written. When it comes in verbally or via text, ask for a photo of the label or the outer box. A single digit difference can change diameter, length, or compatibility.
When you do not have the SKU, force the request into SKU-ready fields: manufacturer, product family, size (diameter and length), platform (coronary vs peripheral vs neuro), and any must-have attributes such as hydrophilic coating, shaft stiffness, or marker configuration. That information narrows the search to a specific family so you can land on an exact catalog number instead of guessing.
Validate the part number against clinical intent
SKU accuracy is necessary, but it is not sufficient. Before you commit to sourcing, validate that the part number matches what the team is trying to accomplish.
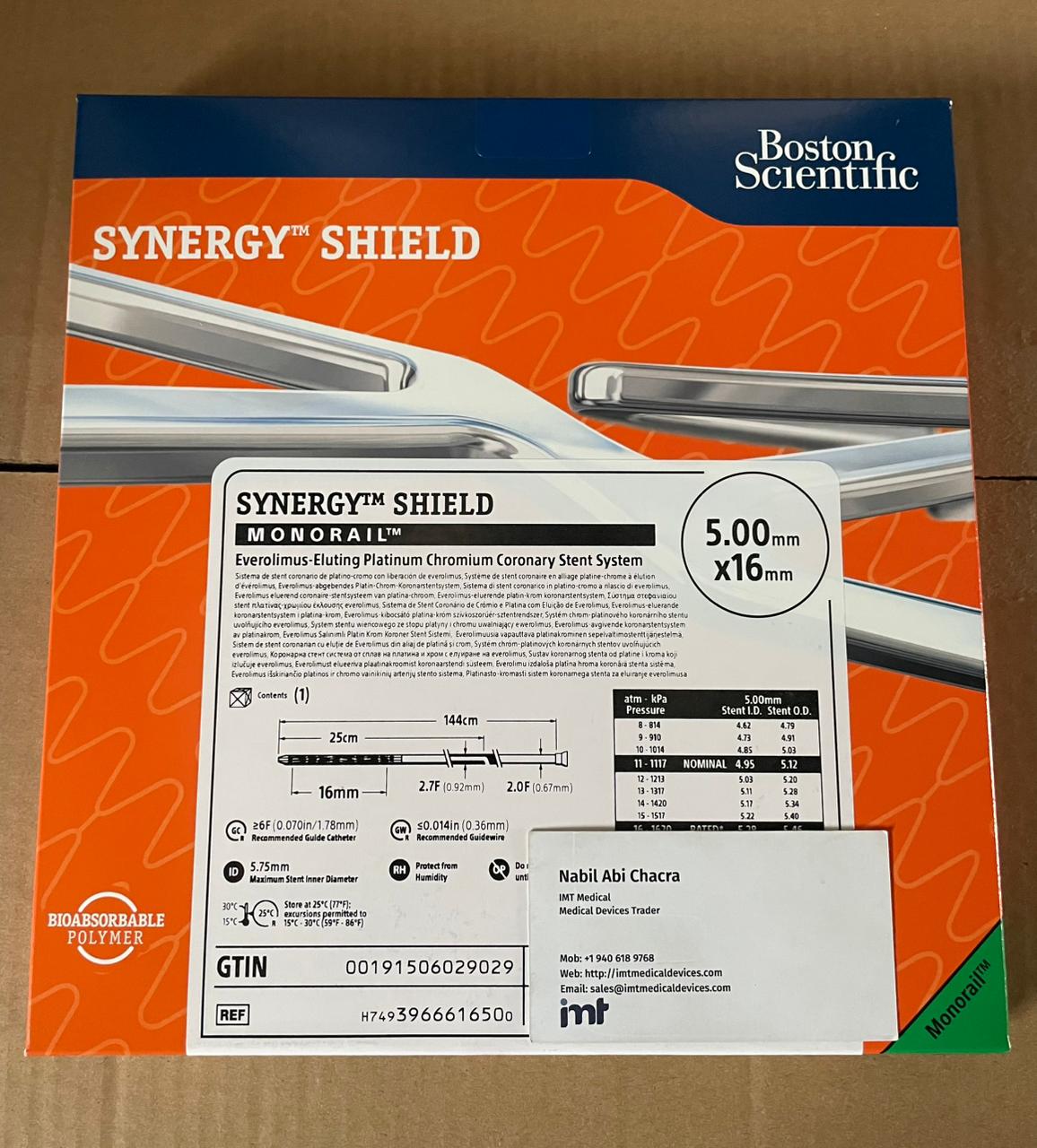
For coronary and peripheral stents, a common mismatch is platform or delivery system generation - “same stent” to the user, different SKU because of a newer system or different compatibility with guides. For balloons, the frequent issues are working length, rated burst pressure, and whether the balloon is semi-compliant or non-compliant. For neurovascular microcatheters and aspiration catheters, inner diameter, distal length, and tip profile can make the difference between “works fine” and “does not track.”
This is also where you confirm packaging and unit-of-measure. Some items are single units; others are sold in boxes with a distributor-specific ordering unit. If your ERP expects a box quantity but the quote is per unit, you will create an avoidable receiving and inventory reconciliation problem.
Use manufacturer family logic to find the right SKU
When a buyer has partial information, family logic is your fastest path to an exact match. Most major manufacturers structure catalog numbers predictably within a product family. A guidewire family might encode length and tip load; a balloon may encode diameter and length; a stent may encode platform, diameter, and length.
The practical move is to anchor on a known “adjacent” SKU from your past purchases and then step to the required size. If your program uses a particular family of coronary balloons, pull a prior PO line and adjust only the parameters you know must change. That approach reduces the chance of drifting into a different family with a different performance profile.
When you are coordinating across service lines, do not assume coronary logic maps cleanly to peripheral logic, and do not assume peripheral logic maps to neuro. Even within the same manufacturer, catalog number patterns can differ by division.
Confirm authenticity and traceability before you chase price
Interventional programs usually care about two sourcing outcomes: correct product, on time. Price matters, but not at the expense of authenticity and traceability.
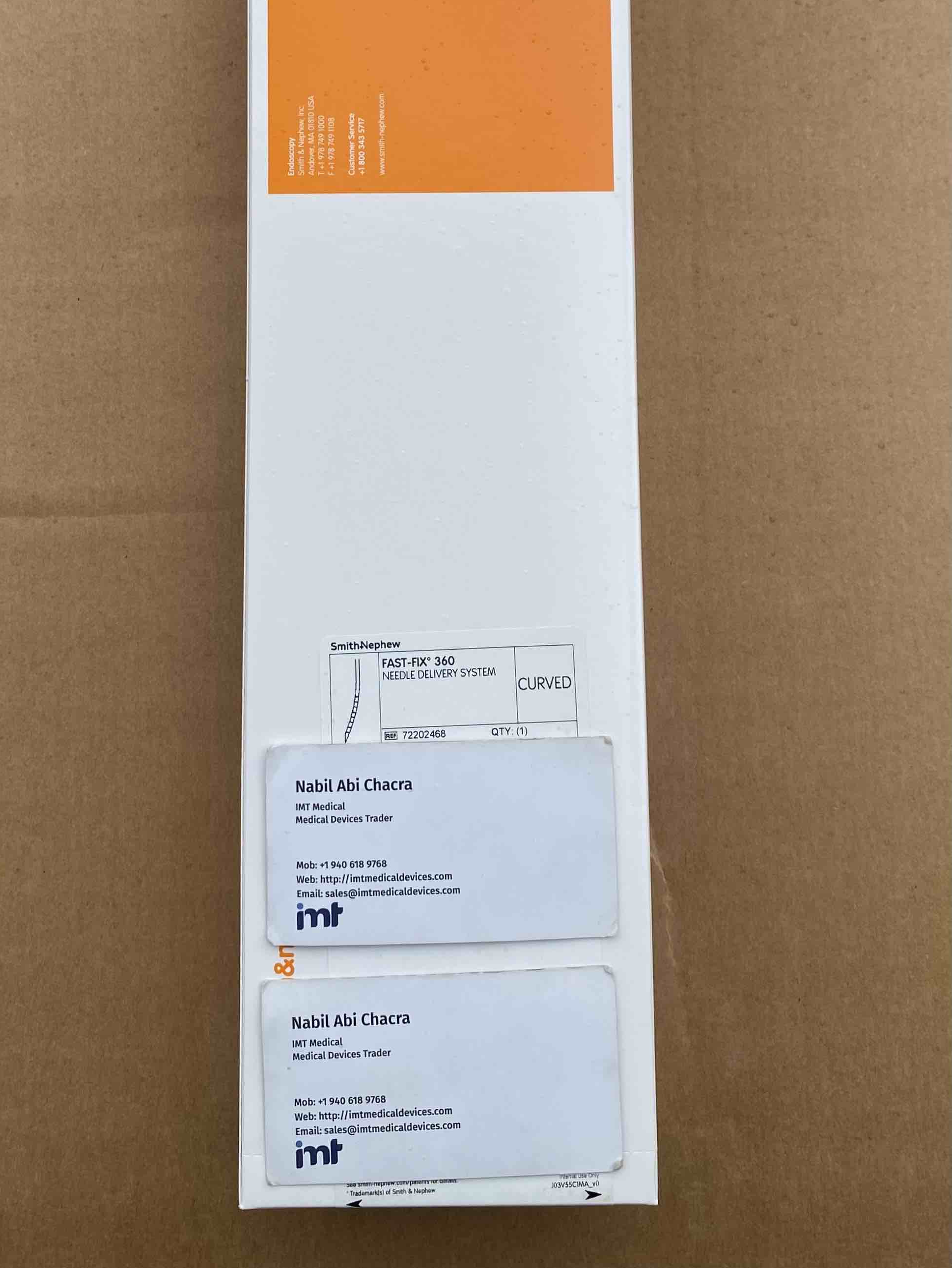
The minimum documentation expectation should include the manufacturer name, the exact catalog number, lot or serial traceability where applicable, and clear expiration dating. If you are exporting or supplying to a facility with strict receiving controls, you may also need country-of-origin, documentation of storage conditions, and confirmation that labeling is acceptable for the receiving market.
If a supplier cannot clearly state what they will ship at the SKU level, or cannot support traceability at receiving, that is not a sourcing win. It is a future nonconformance.
Decide early: exact match, approved equivalent, or case-by-case substitution
The fastest way to burn time is to treat every request as if it must be an exact match, then discover late that equivalents are allowed, or the reverse.
Set a simple rule internally:
- Exact match required for physician preference, standardized platforms, or devices with tight compatibility constraints (common in neurovascular and certain coronary platforms).
- Approved equivalent allowed when your value analysis and clinical leadership have already defined substitutes.
- Case-by-case substitution when supply is constrained and the clinical team is willing to review attributes before approval.
If you are in the case-by-case lane, your sourcing packet should include the requested SKU, the proposed substitute SKU, and a side-by-side of the attributes that matter for that category. Keep it operational, not marketing. The goal is to get a fast clinical yes or no.
Work lead time and allocation reality into the sourcing plan
“Available” can mean many things. It might mean in-stock now, available to ship after internal release, available next month, or available only under allocation.
For high-velocity items like coronary guidewires, guiding catheters, and balloons, you need two dates: ship date and arrival date at dock. For procedure scheduling, arrival at dock is what matters. If you are exporting, add time for documentation prep, handoff, and customs clearance.
If you are seeing repeated constraints in a product family, treat it as a sourcing signal. You may need to increase on-hand safety stock, add a second approved product family, or split purchases across multiple manufacturers if standardization allows.
How to source medical device skus across brands without compatibility mistakes
Cross-brand sourcing is where procurement efficiency can collide with clinical nuance. Consolidating suppliers reduces admin burden, but you still have to protect compatibility at the component level.
Guidewires, balloons, guiding catheters, microcatheters, aspiration catheters, coils, and closure devices each have compatibility considerations that are easy to miss if you only look at the category label. A balloon that fits the lesion is still a problem if the shaft length does not match the guide or access approach. A microcatheter with the right ID can still fail the case if the distal profile does not match the target anatomy.
When you are sourcing multiple components for a program, keep a short “must not change” list per procedure type. For example, your cath lab may be tolerant on guide catheter brands but strict on guidewire family. Your neuro program may be strict on microcatheter families and coil detachment platforms. That reality should drive what you consolidate and what you keep tightly standardized.
This is also where manufacturer breadth matters. If you can source across major brands such as Medtronic, Boston Scientific, Asahi, MicroVention, Terumo Neuro, Terumo, Cordis, Abbott, BD, B. Braun, Ethicon, Smith and Nephew, Coloplast, Beckman Coulter, Roche Reagents, Bio-Rad, and Siemens, you reduce the number of separate sourcing loops you have to run - but only if SKU accuracy stays clean.
Build a repeatable SKU sourcing checklist for each product class
You do not need a 40-field form. You need the few fields that prevent errors.
For coronary and peripheral balloons: diameter, length, working length, compliance type, shaft length, and unit-of-measure are the usual failure points.
For coronary and peripheral stents: platform name, diameter, length, delivery system generation, and MRI/IFU constraints if your facility tracks them.
For guidewires: length, tip load (where applicable), coating type, and whether it is intended for coronary or peripheral use.
For neuro microcatheters and aspiration catheters: distal ID, proximal ID (if relevant), usable length, tip shape/profile, and compatibility with the intended wire or device.
For coils: detachment system, coil type, size, and compatibility with the microcatheter ID.
Write these as your intake prompts so your team collects the right information before the sourcing request hits a supplier.
Use quote workflows to reduce errors, not add steps
A quote is not just a price. It is your SKU-level confirmation layer.
A clean quote process should return the exact catalog number, description, quantity, unit-of-measure, lead time, and any constraints. If the quote comes back with a description that looks right but a catalog number that does not match, treat that as a stop sign.
If you are sourcing for export, make sure the quote and the subsequent sales documents align on the identifiers your receiving team will check. Misalignment between quote, invoice, and packing list is one of the most common reasons shipments get stuck in internal review.
If you want a single catalog that is already organized by interventional categories and major brands, IMTmedicaldevices.com is built around SKU-level browsing and a “personalized offer” quote workflow so procurement teams can request exactly what they need without translating categories into part numbers after the fact.
When it depends: balancing standardization vs continuity
Some programs can standardize aggressively and run lean inventory. Others operate across multiple physicians and complex anatomies where preference variation is the norm. Your sourcing strategy should reflect that.
If your program is highly standardized, focus on tight SKU control, stronger par levels, and fewer substitutions. The trade-off is you may need higher safety stock for constrained items.
If your program has broad preference variation, accept that you will carry more SKUs or you will spend more time sourcing case-by-case. The trade-off is flexibility when a specific SKU is unavailable.
Either way, the operational win is the same: push uncertainty to the front of the process. Collect the right identifiers, validate clinical intent, lock the substitution policy early, and treat documentation as part of the SKU - not an afterthought.
Your best sourcing outcome is not “a device that could work.” It is the exact SKU the team expects, arriving when the patient schedule requires it, with paperwork that clears receiving without a single follow-up email.