Interventional Cardiology Supplies That Match Your Lab
When a physician asks for a specific guidewire by name, they are rarely asking for a “guidewire.” They are asking for a particular feel, tip response, coating behavior, and compatibility with the lab’s standard workup - and they expect it to be on the shelf.
That is the reality behind interventional cardiology supplies procurement. The job is less about learning what a balloon does and more about keeping procedure flow predictable across physicians, shifts, and call coverage. The best purchasing decisions reduce variability, protect standardization, and prevent last-minute substitutions that create clinical friction.
Interventional cardiology supplies: think in procedure kits, not products
Most cath labs buy by category, but they run by workflow. A coronary PCI may involve a guiding catheter, a workhorse wire, a specialty wire, pre-dilation and post-dilation balloons, a drug-eluting stent, and a closure device - plus the small accessories that keep the case moving. If your purchasing process treats each line item as independent, you end up with “in-stock” inventory that still cannot complete a case.
A more reliable approach is to define a few repeatable procedure configurations, then source interventional cardiology supplies to support those configurations at expected case volume. This is where SKU discipline matters. If your lab standard is a specific 0.014 in workhorse wire and a specific NC balloon series, mixing near-equivalents across vendors often creates hidden costs: staff re-training, preference cards that stop matching inventory, and time spent hunting for alternates.
It also depends on how your service line is staffed. Labs with multiple operators and rotating fellows typically benefit from tighter standardization. Programs built around one or two consistent operators may carry a narrower “preference set” but deeper safety stock.
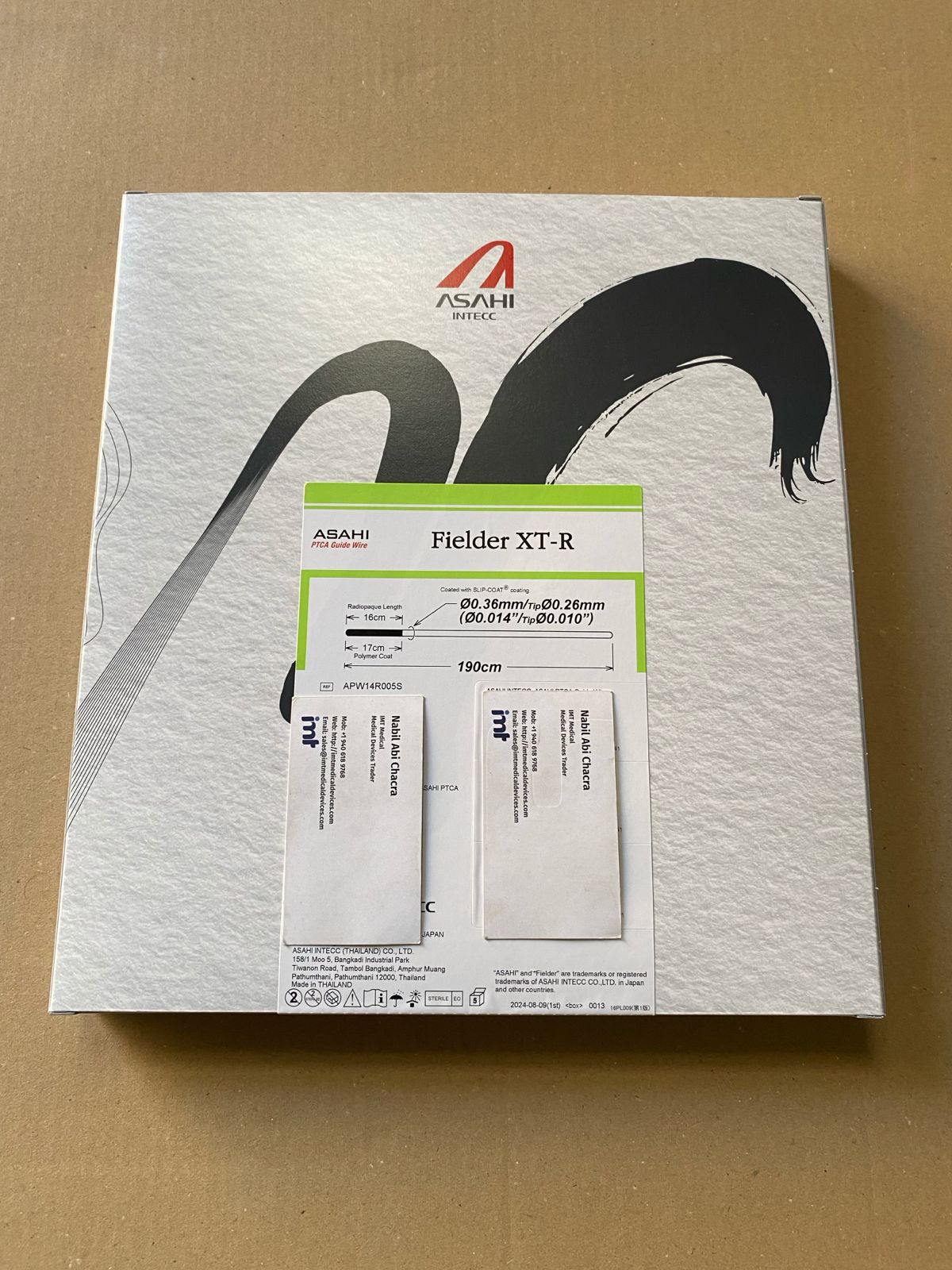
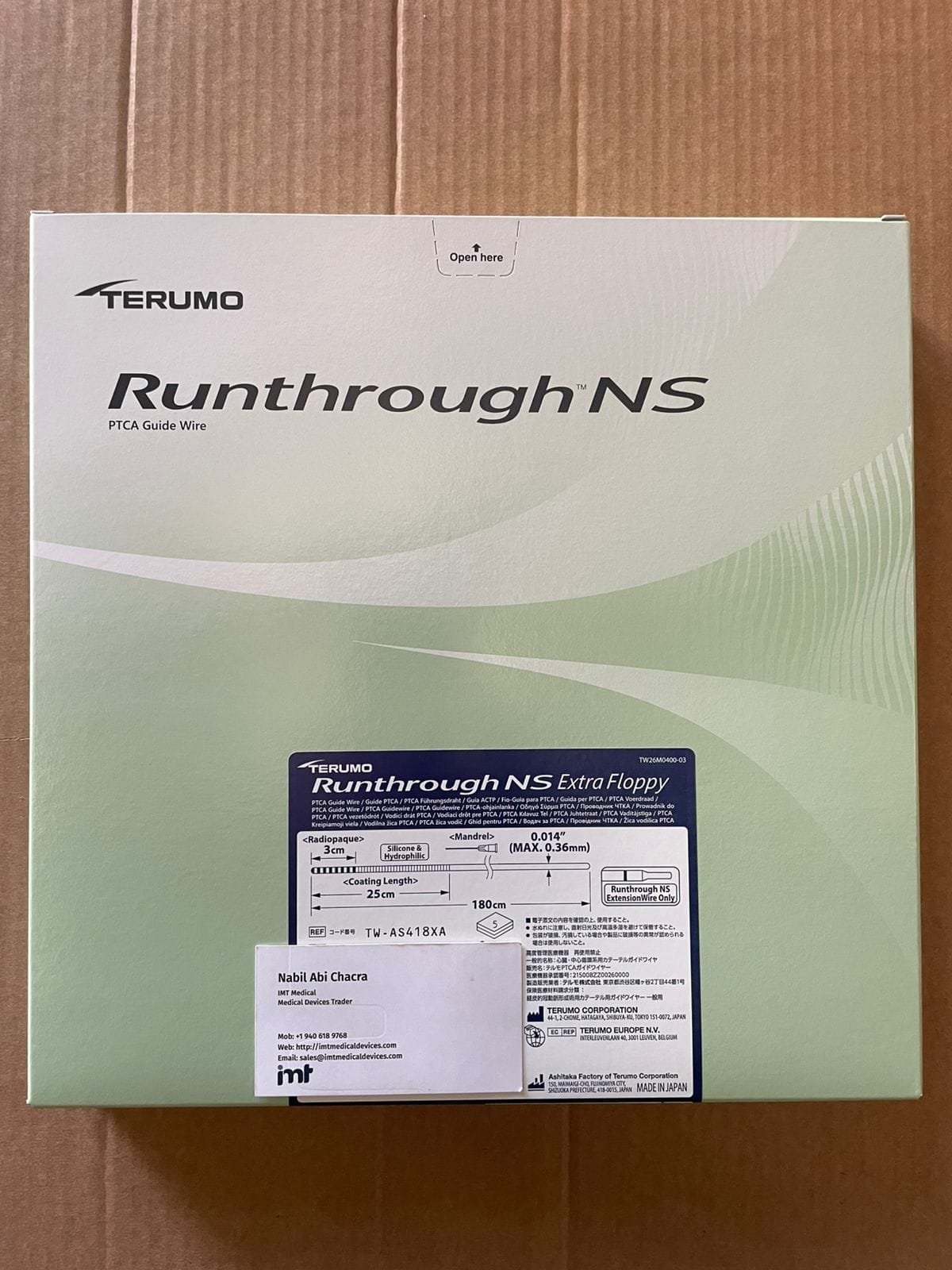
Coronary guidewires: the fastest way to create or remove friction
Guidewires are small, high-impact purchasing decisions. A cath lab can tolerate some variation in syringes or drapes. It usually cannot tolerate variability in wire behavior without pushback.
For coronary inventory, most labs end up with a baseline split: a high-volume workhorse wire for straightforward lesions and a defined set of specialty wires for CTO support, calcified segments, tortuosity, and branch access. The procurement question is not “which wire is best,” but “which wire set keeps physicians productive without stocking ten versions of the same function.”
Practically, this means aligning on a short list by function, then holding the exact part numbers steady. When substitutions happen, they should happen knowingly, not accidentally. If the box shows up and the SKU is off by one character, you have effectively changed the product.
Guiding catheters and diagnostic support: compatibility and consistency
Guiding catheter selection lives at the intersection of operator preference and patient anatomy. From a supply-chain standpoint, the common failure mode is not stocking depth - it is stocking breadth without a plan. You can have many shapes but still miss the one that is actually used daily.
Most labs manage this by identifying a core set of curves and French sizes used for radial and femoral access, then carrying a controlled “long tail” for complex anatomy. Procurement teams typically do best when they keep the core set protected from stockouts and let the long tail be quote-driven.
Compatibility matters here more than marketing. The guiding catheter needs to pair reliably with your guide extension strategies (if used), your wire selection, and your balloon and stent deliverability expectations. If you change one component, you may force changes in others. That is why many service lines prefer to keep consistent families from established manufacturers rather than chasing small unit-cost differences.
Balloon catheters: plan for lesion prep and final optimization
Balloon inventory often grows fastest because it covers multiple functions: pre-dilation, lesion preparation, and post-dilation. The key operational issue is sizing availability. Missing a single diameter or length can slow a case, even if you have “lots of balloons.”
A clean way to manage balloon catheters is to define your standard ranges and keep them complete. Many labs standardize on a primary series for semi-compliant balloons and a primary series for non-compliant balloons, with clear stocking logic for common diameters and lengths.
Trade-offs show up when you decide how many specialty balloons to carry. Some programs prefer to stock niche devices for predictable access and speed. Others keep specialty items quote-based to avoid expiration risk. Both approaches can work, but the choice should be intentional and tied to case mix.
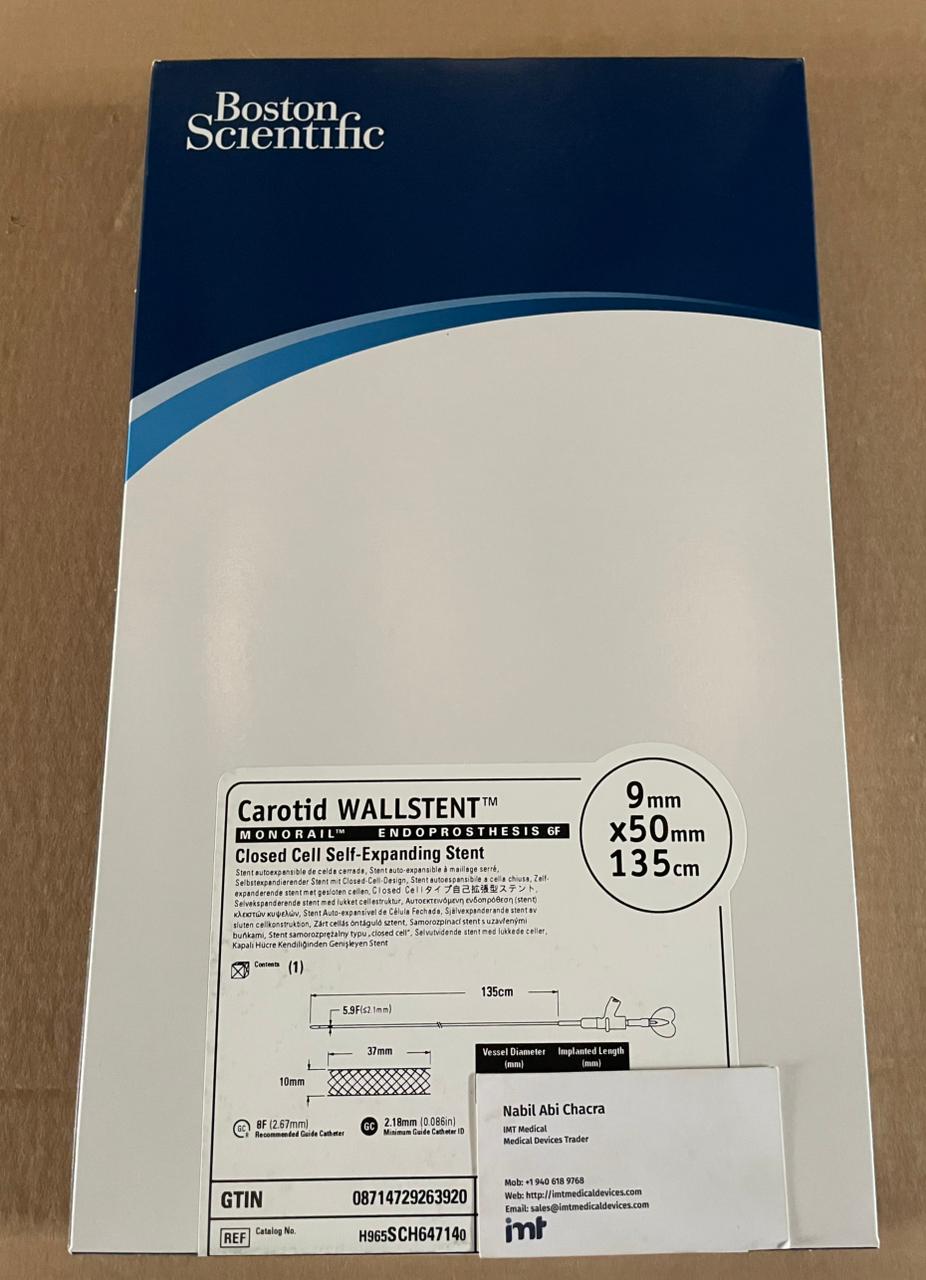
Coronary stents: reduce variability without limiting clinical choice
Stents are where contracting and clinical preference collide. Procurement teams are often balancing physician comfort, hospital agreements, and the need to keep a workable inventory footprint.
Operationally, the stent program should be built around availability of the sizes that actually move. If your shelves are heavy with slow-moving diameters and light on the workhorse sizes, you will still experience backorders that matter.
It helps to treat stents like a sizing matrix with minimums, not a set of “products.” The objective is simple: the right diameter and length should be immediately accessible in the brands your physicians use. When you carry more than one stent platform, the requirement for disciplined replenishment becomes stricter, not looser.
Vascular closure devices and hemostasis: where workflow meets throughput
Closure is a throughput tool as much as a device category. If you are short on your standard closure device, you do not only change the last five minutes of a case. You change recovery time, staff workload, and sometimes access strategy.
For purchasing, the practical questions are: which closure devices are used for femoral access in your program, which are used after larger bore work, and what backup method is acceptable when the standard device is unavailable. The “backup” should be stocked and trained, not theoretical.
Here again, SKU accuracy matters. Many closure device families include multiple variants that look similar at a glance but are not interchangeable. Procurement teams reduce errors by matching the exact manufacturer identifiers, storing in clearly labeled bins, and enforcing lot and expiration rotation.
Adjacent procedural inventory: what you do not want to discover mid-case
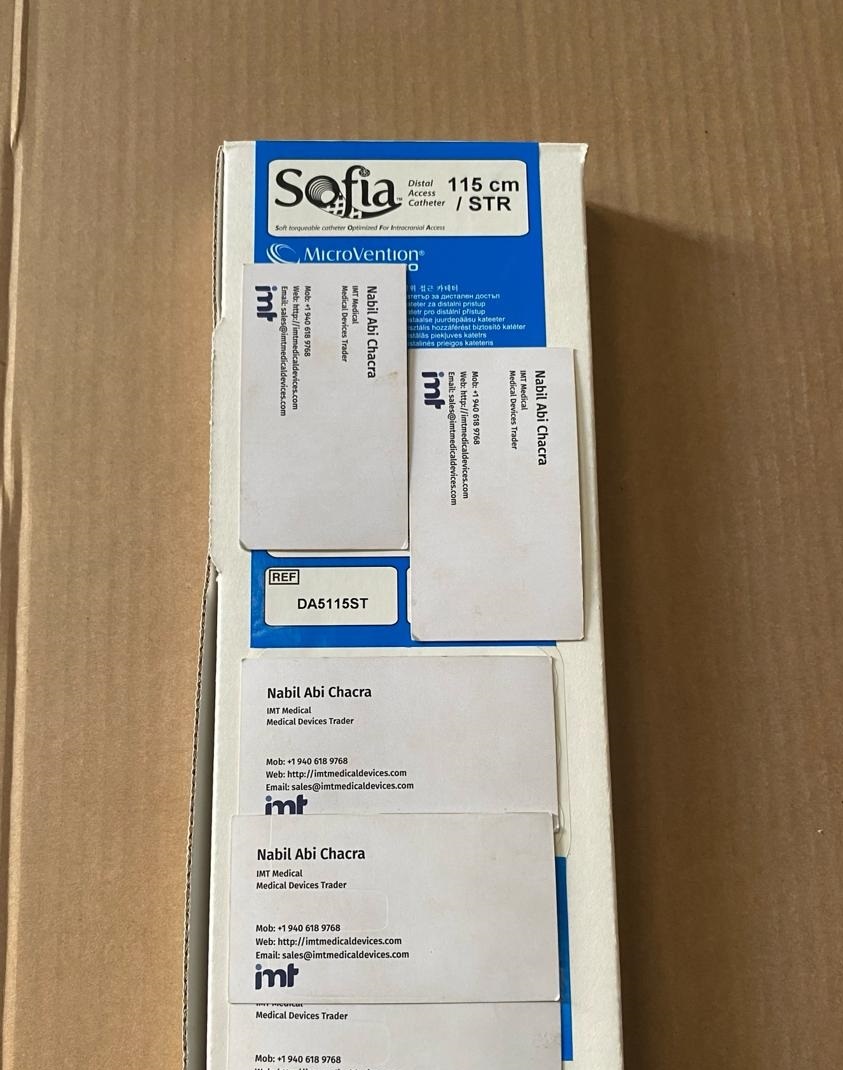
Interventional cardiology supplies do not stop at coronary. Many cath labs and hybrid programs overlap with peripheral and neurovascular inventory, especially for aspiration catheters, microcatheters, coils, and support catheters used in cross-coverage environments.
If your organization runs peripheral vascular or neurointerventional cases through related supply channels, consolidation can reduce friction. A single vendor that can source across major manufacturers can simplify approvals and reduce the number of separate quote cycles - as long as the vendor can provide exact branded SKUs and consistent export documentation when needed.
Manufacturers commonly requested in high-acuity programs include Medtronic, Boston Scientific, Asahi, MicroVention, Terumo Neuro, Terumo, Cordis, Abbott, BD, B. Braun, Ethicon, Smith and Nephew, Coloplast, Beckman Coulter, Roche Reagents, Bio-Rad, and Siemens. The point is not the logo on the box. The point is that most labs have standardized preference cards and compatibility assumptions built around these established product families.
How to buy interventional cardiology supplies with fewer surprises
The fastest way to create purchasing risk in a cath lab is to treat “equivalent” as “the same.” When clinical stakeholders request a part number, it is typically because past substitutions caused delays, deliverability issues, or simply distrust.
A procurement workflow that holds up under pressure tends to include four behaviors.
First, capture exact identifiers early. That means the full product name, reference number, and any configuration notes like length, French size, coating, or tip type. If a physician gives a nickname, convert it into a reference number before the quote request is submitted.
Second, purchase as systems. If you standardize a wire and a balloon series because they perform together, do not source them independently without checking the downstream effect. Small changes compound.
Third, use inventory policy that matches case urgency. High-volume coronary consumables should be stocked to prevent weekend and overnight gaps. Slow-moving specialty items are often better managed with controlled lead times and a clear escalation path for urgent cases.
Fourth, keep substitutions explicit and documented. When backorders happen, the best outcome is not “we found something close.” The best outcome is “we confirmed the alternate with the operator and updated the preference list for this case only.”
If your team is building a consolidated sourcing approach across coronary, peripheral, and neurovascular categories, IMTmedicaldevices.com is structured for SKU-driven browsing and quote-based purchasing across multiple major brands, which can help reduce the time spent splitting orders across vendors.
The procurement metrics that actually reflect cath lab reality
Cath lab supply performance is not only about unit price. The metrics that tend to matter most are fill rate on the exact SKU, time to quote for non-stock items, substitution rate, and expired inventory value. Those metrics align with what clinicians feel: cases start on time, carts are complete, and staff are not improvising.
If you want a single internal checkpoint, use a simple question: can your current interventional cardiology supplies inventory complete tomorrow’s schedule without workarounds? When the answer is consistently yes, the lab runs quieter - and your purchasing team spends less time firefighting and more time improving continuity.