Most Used Cath Lab Disposable Items by Case Type
A cath lab rarely runs out of the “big ticket” implant on the shelf. What stops cases is almost always a disposable: the one guidewire size that matches the operator’s habit, the right hemostasis valve, the Y-connector that fits the setup, or the closure device the team is credentialed on. If you manage inventory for high-acuity interventions, the fastest way to reduce delays is to organize purchasing around the most used cath lab disposable items by procedure type, then standardize the supporting accessories that get consumed every single case.
This is a procurement-oriented view of what moves most in interventional cardiology, peripheral, and neurovascular labs - with practical “what to stock” thinking, brand-level expectations, and the trade-offs that impact utilization.
What “most used” really means in a cath lab
“Most used” is not the same as “most expensive,” and it is not always “highest clinical priority.” In practice it means the disposables that are:
- Opened early in the case (so substitutions cause immediate delay)
- Operator-specific (preference-driven, harder to interchange)
- Needed in multiple procedure families (coronary plus peripheral, or diagnostic plus intervention)
- Consumed regardless of outcome (even if a case converts or aborts)
It also depends on your case mix. A lab that is heavily coronary will burn through diagnostic and guiding catheters, coronary guidewires, balloons, and closure. A peripheral-heavy lab may consume more long sheaths, hydrophilic wires, PTA balloons, and re-entry or atherectomy adjuncts. Neurovascular centers lean into microcatheters, microwires, aspiration catheters, and coils.
Most used cath lab disposable items in coronary cases
Diagnostic and guiding catheters
For coronary workflows, diagnostic catheters and guiding catheters are among the highest-turn disposable lines. They are opened almost immediately, and catheter shapes are tied to operator technique and access approach.
Typical ordering patterns are driven by access preference (radial vs femoral), catheter curve family, and French size. Even when you can substitute, the practical cost is time and frustration, so buyers tend to keep the “usual curves” deep.
Common manufacturer families used globally include offerings from Medtronic, Boston Scientific, Terumo, Cordis, and Abbott. The key procurement variable is breadth: stocking a narrow set can reduce expiration risk, but it increases the odds of an operator-specific miss.
Coronary guidewires
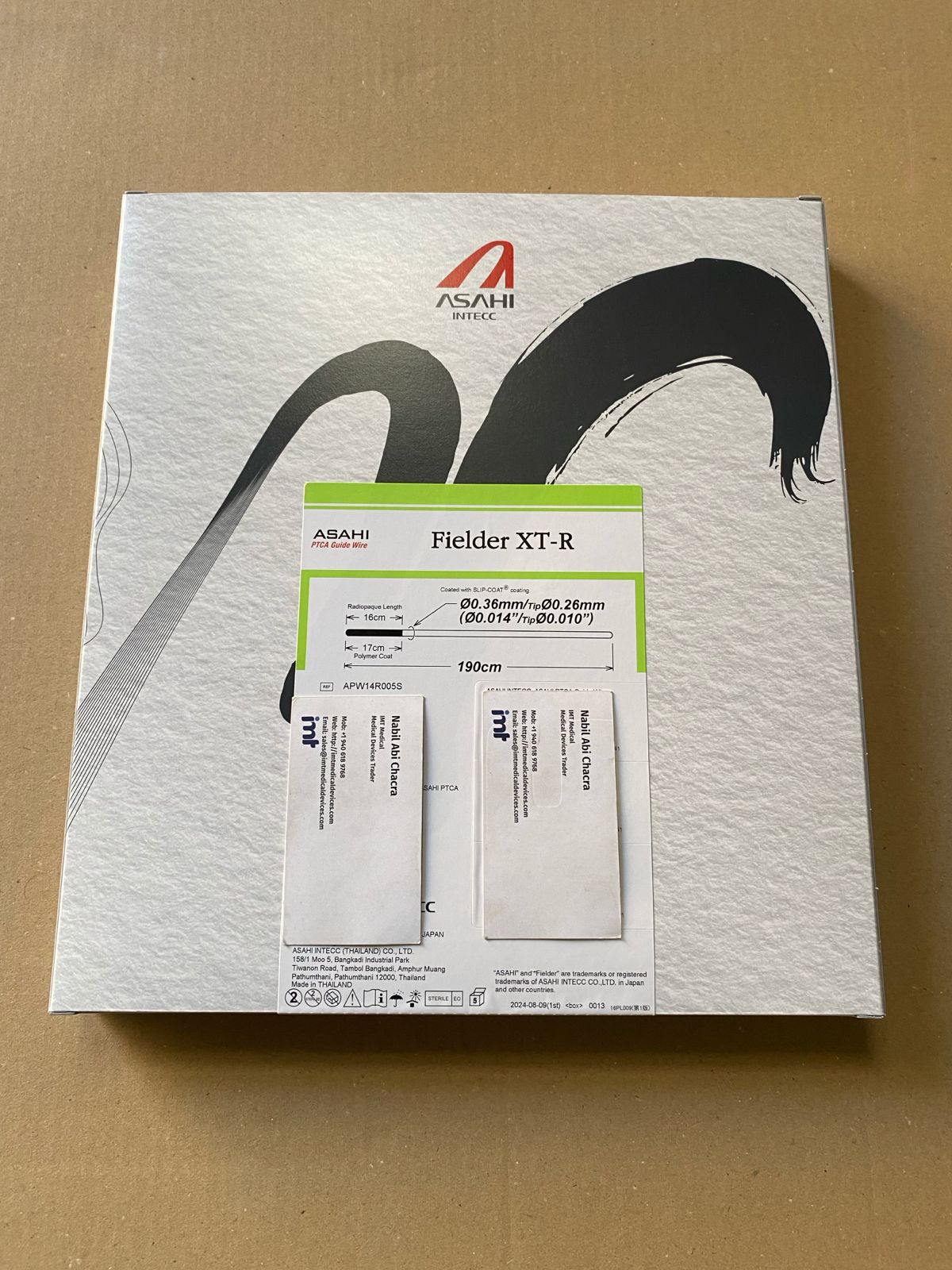
Coronary guidewires are high-consumption because most PCI cases open at least one, and complex lesions may require multiple wires. The “most used” wires typically include a general workhorse plus at least one more supportive or specialty option.
Asahi is a frequent preference brand in many labs due to predictable handling across lesion subsets. That said, utilization depends on your operators and the complexity profile of your coronary population.
For purchasing, it helps to map demand to three buckets: workhorse, support/escalation, and specialty (CTO, extreme tortuosity, heavily calcified lesions). If you only stock for routine lesions, your team will open two or three wires per complex case trying to replicate a missing profile.
Balloons (PTCA and specialty)
Pre-dilation, post-dilation, and stent optimization create steady balloon demand. PTCA balloon sizes skew toward your stent platform usage and vessel sizing habits, while non-compliant balloons see high use in optimization-heavy practices.
The trade-off is SKU sprawl. Balloon sizing produces a combinatorial inventory problem, so most procurement teams rationalize by:
- Stocking high runners in common diameters and lengths
- Carrying limited “edge sizes” (very small or very large) as safety stock
- Separating standard-compliance inventory from non-compliant optimization inventory
Suppliers commonly requested include Boston Scientific, Medtronic, Terumo, and Abbott, with selection driven by deliverability, rated burst pressure expectations, and trackability.
Coronary stents
Drug-eluting stents are not “consumed” at the same rate as small accessories, but they remain among the most frequently opened implantables in coronary labs. Because stents tie up capital and carry expiration risk, many facilities balance on-hand depth with rapid replenishment.
Purchasing typically aligns to a primary platform and a secondary option for specific anatomy or sizing gaps. The operational risk is not simply being out of stents - it’s being out of the exact diameter/length the operator wants at the end of a case.
Hemostasis valves, Y-connectors, and torque devices
These items are consistently “most used” because they are procedure-agnostic within coronary work and are opened routinely. They are also easy to overlook because they are inexpensive compared to wires and balloons.
From a supply-chain standpoint, these are ideal for standardization. Fewer SKUs, consistent compatibility, and stable usage make them predictable reorder lines.
Contrast, syringes, stopcocks, and transducer accessories
Depending on your facility’s split between cath lab stock and central supply, contrast and injection-related disposables can be among the highest-volume consumables. Some labs include manifold kits, pressure tubing, and stopcocks in procedure packs; others order separately.
What matters for procurement is ensuring compatibility with your injector setup and your chosen manifold workflow. Switching brands may be clinically acceptable, but it often creates setup variation that staff will resist.
Vascular closure devices
Closure utilization is driven by access site strategy. Radial programs use fewer femoral closure devices, while femoral-heavy or large-bore practices will consume closure at a high rate.
Because closure devices are operator-credentialed and technique-specific, substitutions are harder than with basic disposables. Many labs keep a primary closure device and a backup option for anatomy or anticoagulation scenarios.
Major manufacturers in this space include Abbott, BD, and Terumo, among others, with selection influenced by sheath size range, learning curve, and complication management preferences.
Most used disposable items in peripheral interventions
Sheaths and introducers (including long sheaths)
Peripheral cases commonly consume more sheath variety than coronary cases, especially when working below the knee or navigating tortuous iliac anatomy. Long sheaths and supportive access systems are opened frequently.
The procurement challenge is that peripheral requires both diameter and length planning. Stock too shallow and you stall cases; stock too broad and you increase expiry exposure.
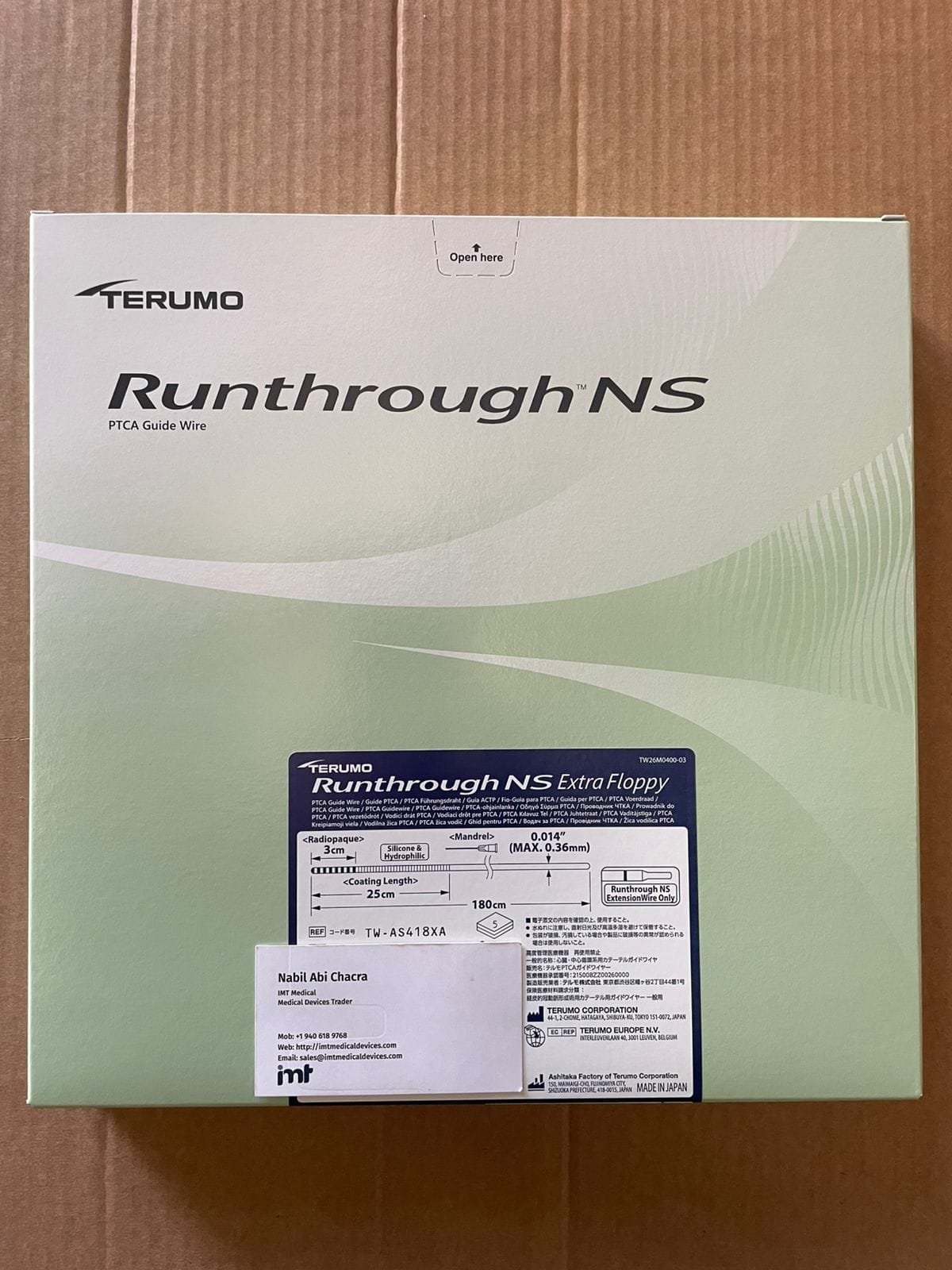
Hydrophilic guidewires and support wires
Peripheral wiring is a high-burn category. Hydrophilic-coated wires are common first-line tools for crossing, with stiffer support wires opened as escalation.
Terumo is often requested for hydrophilic wire performance, while other brands fill support and specialty roles. Demand depends on how aggressive your operators are in crossing attempts and how often you treat chronic occlusions.
PTA balloons and specialty balloons
PTA balloons move quickly in peripheral programs, especially where balloon angioplasty is first-line. Specialty balloons (such as drug-coated balloons) also drive consumption, but availability and local policy can affect usage.
From a purchasing viewpoint, the question is whether your team wants broad choice on the shelf or a streamlined set with dependable replenishment. Peripheral balloon SKUs multiply quickly, so many buyers set minimum/maximum levels by territory (iliac, fem-pop, BTK).
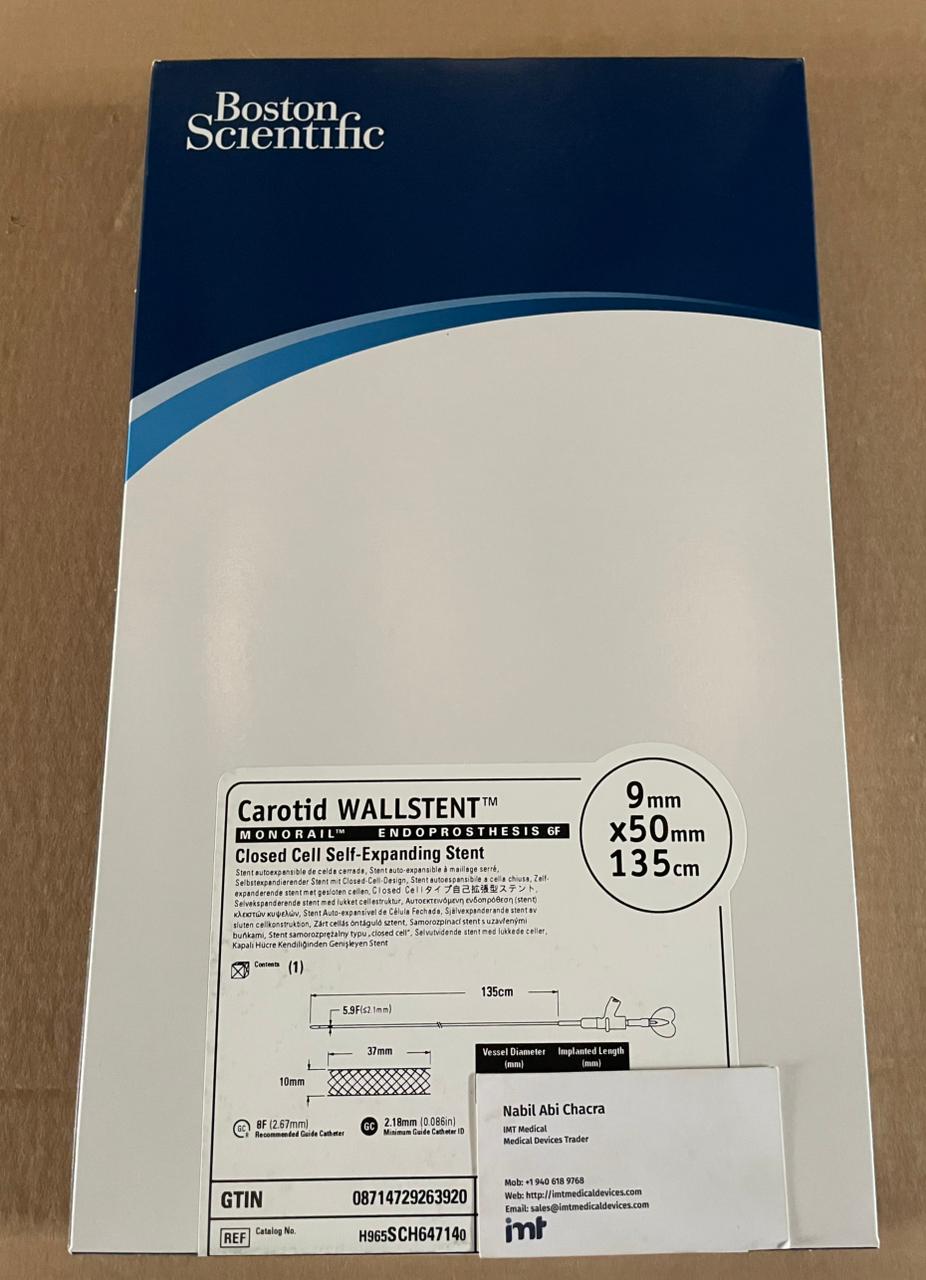
Peripheral stents and covered stents
Peripheral stent use varies widely by physician preference and lesion location. Covered stents and specialty implants can be “must have” for bailout scenarios, which changes stocking logic: you may not open them often, but when you need them, you need them immediately.
This is a classic “it depends” category where inventory is justified by risk tolerance and transfer time, not just average monthly usage.
Most used disposable items in neurovascular cases
Neuro cases consume fewer basic coronary-style items and far more micro-scale devices, often opened in sequence as the plan evolves.
Microcatheters and microwires
Microcatheters and microwires are foundational and frequently opened. Selection is driven by target anatomy, support requirements, and device compatibility (coils, stent retrievers, flow diverters).
Terumo Neuro and MicroVention are commonly specified in neuro programs for microcatheter and neuro device ecosystems. Stocking needs to reflect your dominant case types: aneurysm coiling, thrombectomy, AVM work, or flow diversion.
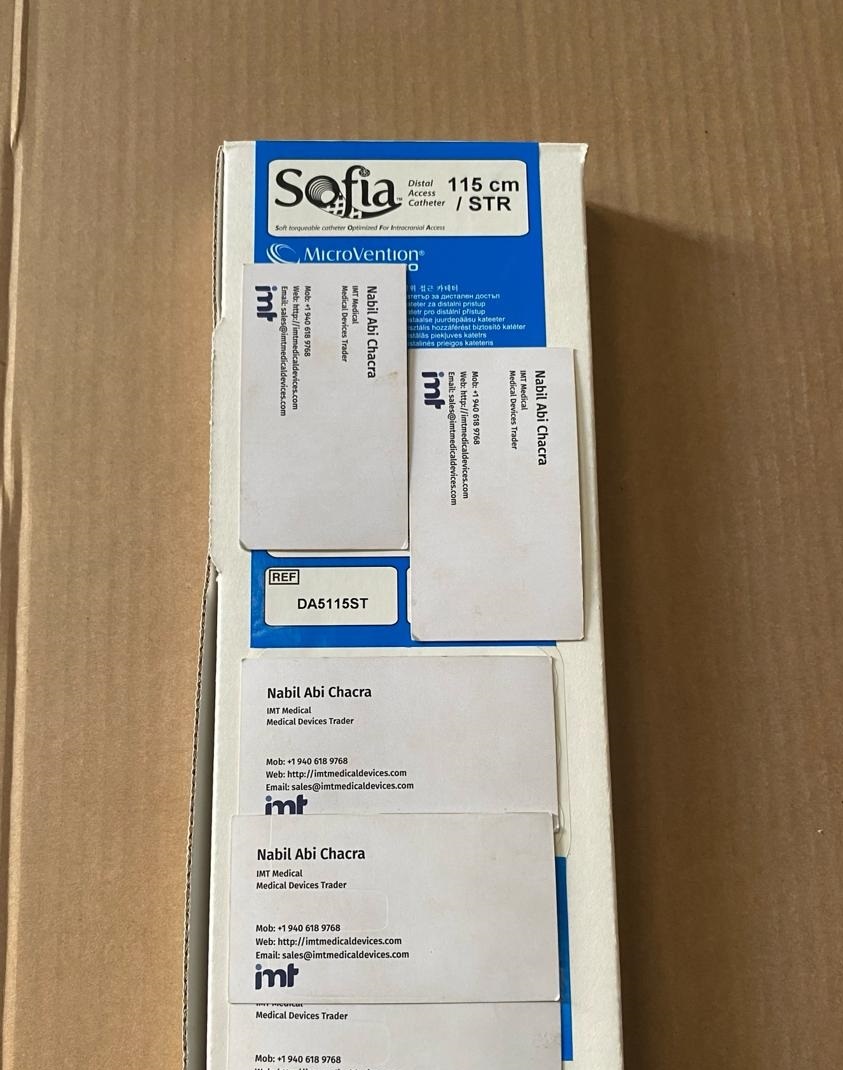
Aspiration catheters and thrombectomy consumables
In stroke thrombectomy, aspiration catheters and associated tubing/components can be among the most used items. The reality is that thrombectomy workflows are time-critical, so facilities prioritize on-shelf availability of the exact catheter family the team uses.
The procurement trade-off is expiration and capital tie-up versus the operational cost of not being able to run a stroke case without delays.
Coils and adjunct embolization products
Coils are case-dependent but can be high-volume in aneurysm programs. They also carry significant SKU complexity (diameter, length, softness profiles). Neuro teams frequently require specific coil families, so substitution is not always acceptable.
How to stock the “most used” without drowning in SKUs
The fastest procurement wins usually come from separating your inventory into two layers: core runners and preference-driven specialties.
Core runners are the items that get opened in most cases: standard diagnostic/guiding catheters, common guidewires, common balloon sizes, routine hemostasis valves, and your primary closure approach. These are the lines that should have clear min/max levels and predictable reorder triggers.
Preference-driven specialties include CTO wires, unusual catheter curves, edge balloon sizes, bailout covered stents, and neuro microcatheters that only one physician uses. These should be stocked intentionally - either as limited safety stock, on-demand ordering, or held as consignment where available.
If you operate across multiple countries (for example in Gulf, Latin America, or parts of Asia), one more variable matters: lead time volatility. When lead times are inconsistent, it is rational to carry slightly deeper stock of high-velocity disposables, even if it increases expiry management work.
Brand availability and sourcing realities buyers plan around
Most cath labs prefer branded, familiar platforms because device behavior matters in tight anatomy and complex lesions. Procurement decisions often come down to two operational questions: can you supply the exact requested manufacturer line, and can you repeat that supply consistently.
Facilities and competing distributors that source outside local channels often prioritize access to major brands such as Medtronic, Boston Scientific, Asahi, MicroVention, Terumo Neuro, Terumo, Cordis, BD (Becton Dickinson), BBraun, Ethicon, and Abbott. The practical value is reduced substitution risk and fewer mid-case workarounds.
If your purchasing team is building a second supply lane, keep documentation tight: item descriptions, reference numbers, and packaging configurations should match what your cath lab staff expects to receive and open.
For buyers who need a broad branded catalog across coronary, peripheral, and neurovascular categories with quote-driven fulfillment, IMTmedicaldevices.com is structured for fast product discovery by manufacturer and device family.
Closing thought
If you want fewer case delays, don’t start by asking which implants are “best.” Start by tracking which disposables get opened in the first 10 minutes of your most common procedures - then make those lines boringly available, week after week.