Coronary Intervention Procedures Explained
When a cath lab schedules a PCI list, procurement errors show up fast. Coronary intervention procedures depend on exact device compatibility, physician preference, and reliable access to branded inventory across guidewires, balloons, stents, catheters, and adjunctive products.
For buyers, the issue is not defining PCI at a basic level. It is maintaining supply continuity for clinically routine but operationally demanding cases. A standard lesion, a bifurcation, heavy calcification, thrombus burden, chronic total occlusion, or bailout support all change the product mix. That means sourcing decisions need to reflect how coronary intervention procedures are actually performed, not just how categories appear in a catalog.
What coronary intervention procedures require from a supply perspective
In practical terms, coronary intervention procedures are built around vascular access, lesion crossing, vessel preparation, stent delivery when indicated, and post-deployment optimization. Each stage has direct procurement implications because a complete procedure is never one SKU. It is a set of interoperable products that must be available in the right sizes, lengths, profiles, and brand families.
A routine case may require a guiding catheter, a coronary guidewire, a pre-dilatation balloon, a drug-eluting stent, and a post-dilatation balloon. More complex anatomy often expands that requirement to include specialty wires, micro catheters, support catheters, aspiration devices, or additional balloons for lesion modification and final optimization.
This is where many purchasing teams face a trade-off. Standardization can improve purchasing efficiency and simplify shelf management, but over-standardization may reduce operator flexibility. In coronary work, preference matters. Many interventional cardiologists build case strategy around familiar wire behavior, catheter support, crossing performance, and deliverability characteristics from specific manufacturers.
Core product categories used in coronary intervention procedures
From a wholesale and inventory planning standpoint, coronary intervention procedures typically center on several product groups.
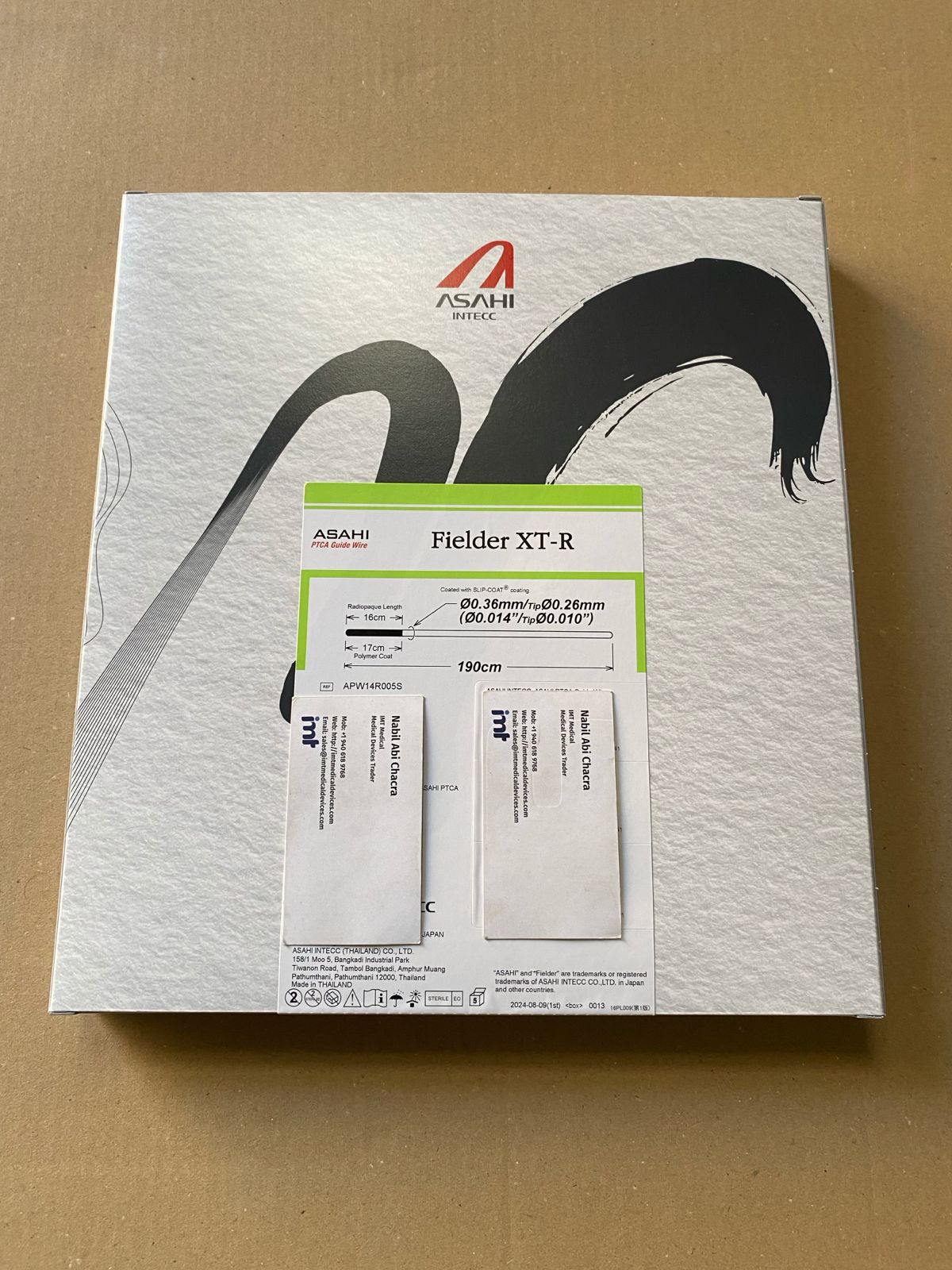
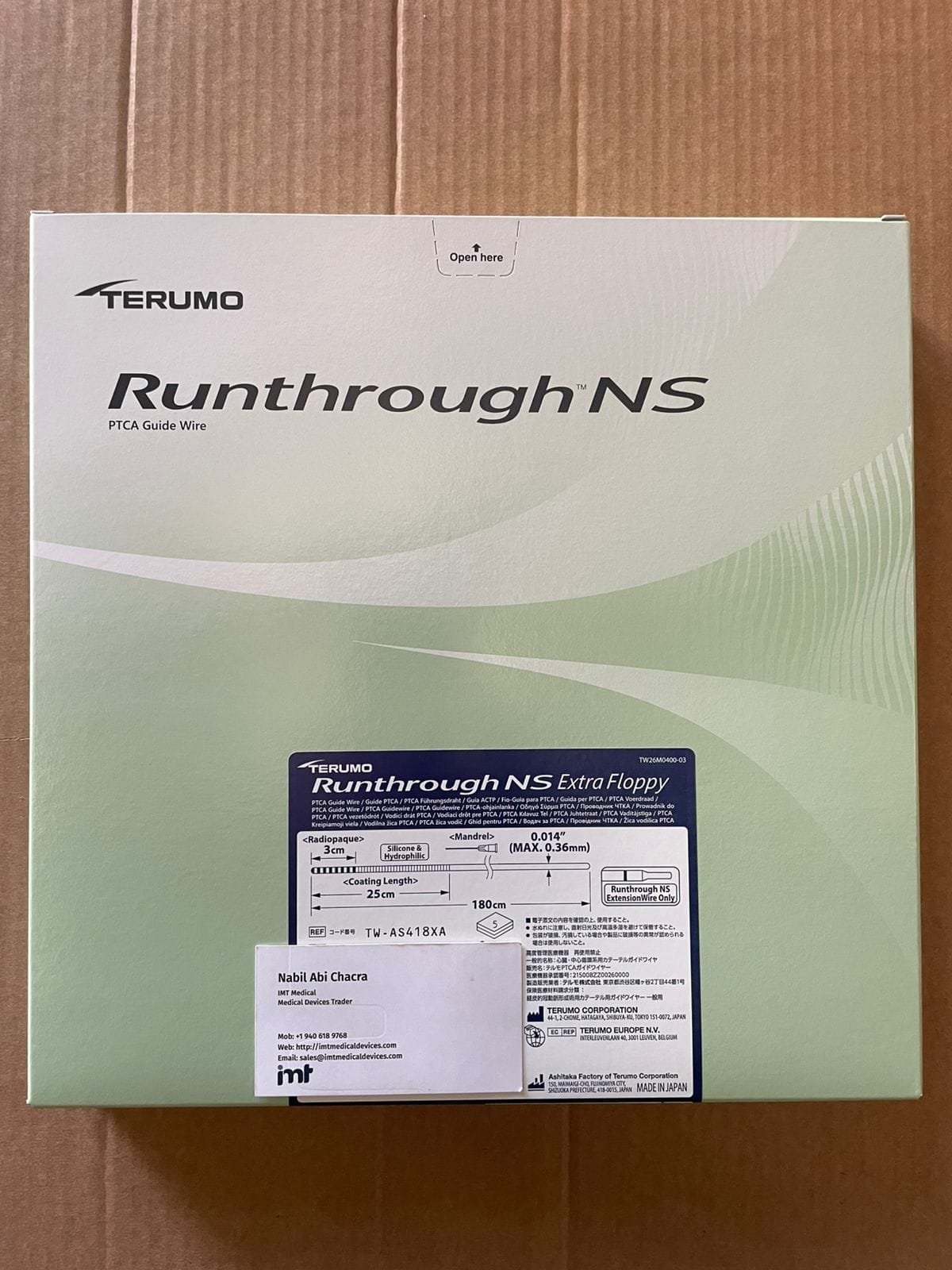
Guidewires and crossing support
Guidewires are often the first preference-sensitive decision in the case. Buyers usually need a mix rather than a single platform, because workhorse wires, hydrophilic wires, and specialty wires serve different lesion and vessel demands. In more difficult anatomy, micro catheters and support catheters become relevant for wire exchange, torque response, and crossing support.
For procurement teams, this means stocking to the actual complexity profile of the facility. A center doing high-volume routine PCI will not mirror the needs of a lab managing more CTO, calcified, or tortuous lesions.
Balloons for preparation and optimization
Balloons cover more than pre-dilatation. Coronary intervention procedures may involve semi-compliant balloons for initial preparation, non-compliant balloons for precise post-dilatation, and specialty balloons depending on lesion characteristics and operator technique.
The main supply issue is width and length availability. Gaps in balloon matrix can delay treatment choices inside the procedure room. Buyers usually benefit from reviewing utilization by diameter, length, shaft preference, and crossing profile rather than treating balloons as a broad interchangeable class.
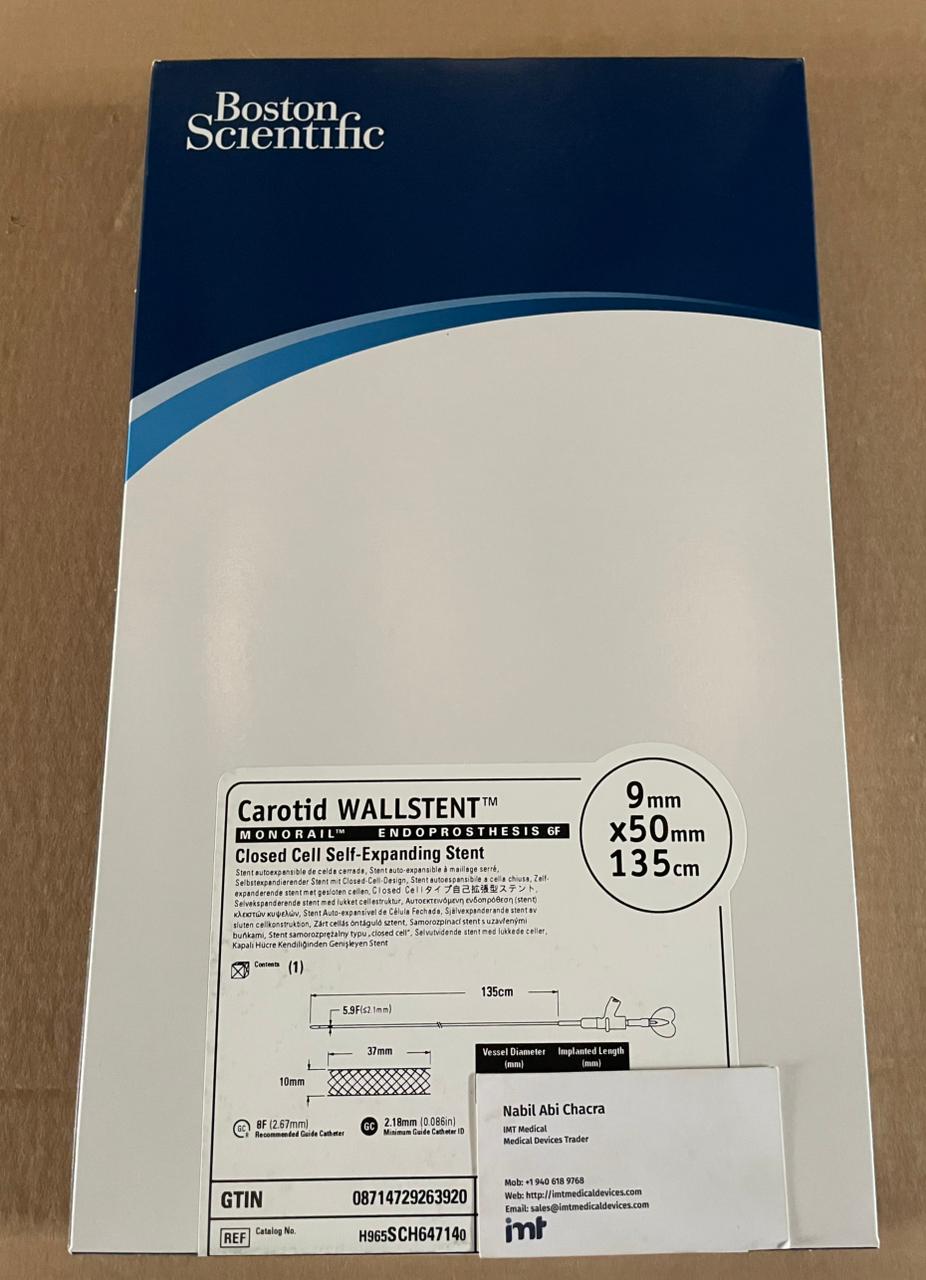
Coronary stents
Drug-eluting stents remain central to many coronary intervention procedures. Here, procurement decisions are influenced by platform familiarity, radial strength, deliverability, lesion coverage requirements, and local clinical preferences. Brand continuity is often a priority because interventional teams prefer consistency in deployment feel and expected performance.
The challenge is balancing breadth with turnover. Too narrow a stent inventory can create case limitations. Too broad a portfolio can tie up capital in slow-moving sizes. The right mix usually comes from historical use patterns, physician preference mapping, and expected case complexity.
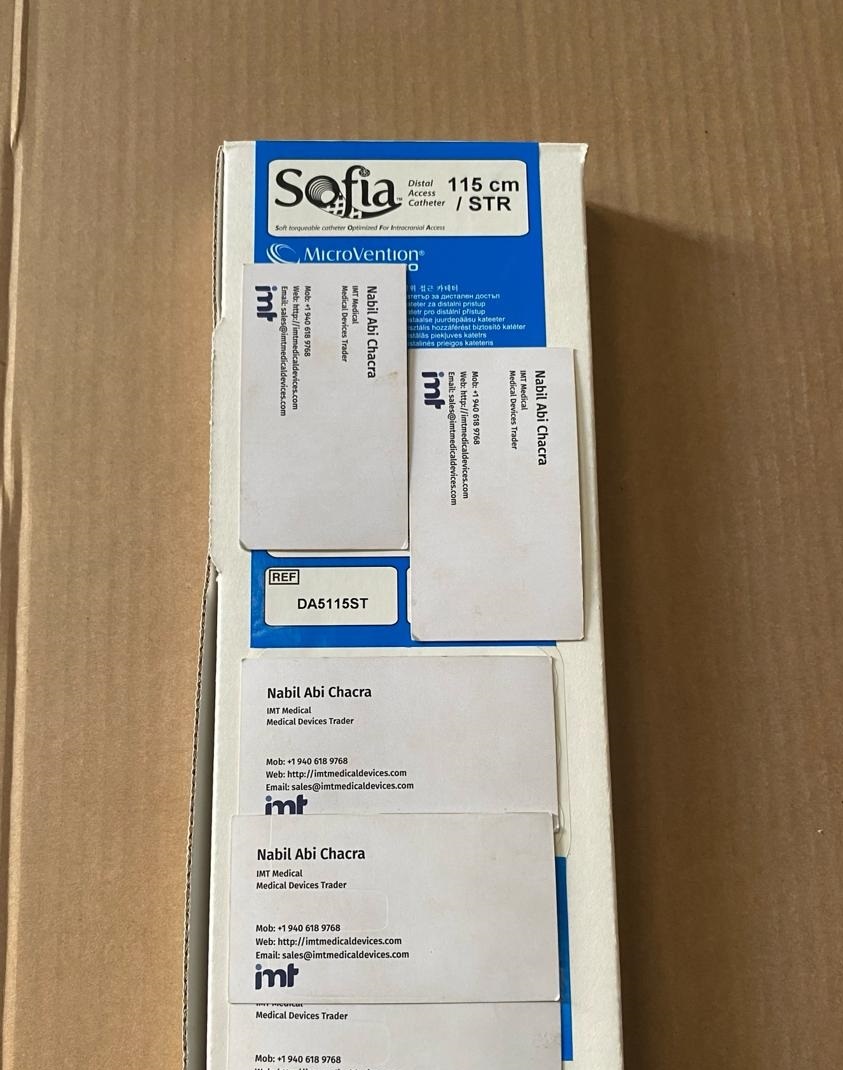
Guiding catheters and access-related devices
Guiding catheter selection affects backup support, device delivery, and procedural efficiency. Radial-first centers may have a different inventory pattern than femoral-heavy labs, and even within radial practice, shape preference can vary significantly by operator.
This category is sometimes underestimated during procurement reviews because it is treated as routine stock. In reality, stockouts in high-use guide shapes can affect throughput immediately.
Adjunctive and bailout devices
Not every case needs aspiration catheters or additional support devices, but some labs cannot afford not to have them available. Coronary intervention procedures do not always follow the original treatment plan. Thrombus, dissection, underexpansion, or access-related variation can shift requirements quickly.
For that reason, buyers often need a practical strategy for lower-volume but clinically important SKUs. The objective is not maximum inventory in every category. It is dependable access when the case stops being routine.
Why brand recognition matters in coronary procurement
In interventional cardiology, branded device sourcing is not only a preference issue. It is a risk management issue tied to familiarity, training, and expected product behavior. Buyers serving experienced operators know that equivalent category labels do not always mean equivalent handling.
A coronary wire from one manufacturer may be selected for trackability and tactile response, while another is chosen for penetration or support. The same applies to balloon pushability, stent deliverability, and catheter backup. For this reason, procurement teams commonly align with recognized manufacturers such as Terumo, Asahi, Boston Scientific, Medtronic, Abbott, and Cordis where product behavior is already understood by the clinical team.
There is also a practical export consideration. In international procurement, recognized brands can simplify internal approval and adoption because clinicians and administrators already know the product family. That shortens evaluation cycles compared with unfamiliar alternatives.
Planning inventory for different coronary case profiles
A facility performing mostly straightforward PCI has a very different stocking model from a referral center handling complex coronary intervention procedures. Buyers should avoid using a single template across both environments.
Routine PCI programs typically need depth in fast-moving guidewires, standard guiding catheter shapes, common balloon sizes, and high-turnover stent diameters and lengths. Complex coronary programs usually require more breadth, including specialty wires, more varied support options, and additional lesion-specific devices.
There is a cost trade-off here. Holding broad inventory improves responsiveness but increases carrying burden and expiry exposure. Lean stocking reduces tied-up capital but can create case delays and fragmented purchasing. The better answer often sits in between: strong local stock for core SKUs, with a responsive supply partner for replenishment and harder-to-source branded lines.
Common procurement risks in coronary intervention procedures
The biggest risks are usually operational, not theoretical. SKU mismatches, discontinued references, partial brand substitution, and weak forecasting can all affect case readiness.
A common problem is assuming cross-brand interchangeability without checking operator acceptance. Another is sourcing by category name only, without confirming exact size matrix and compatibility requirements. This may look acceptable during purchasing review but fail in real use.
International buyers also need to watch lead times, export documentation, packaging integrity, and consistency across shipments. In coronary intervention procedures, one missing size or one unsupported brand change can disrupt a case cart more than a broad shortage in a less specialized department.
What buyers should evaluate in a coronary supply partner
For this category, price matters, but it is rarely the only decision point. A useful supplier should support exact product identification, recognized brands, and continuity across multiple interventional categories. That is especially relevant for organizations trying to consolidate sourcing across coronary, peripheral, neurovascular, and laboratory procurement.
Buyers should also look at whether the supplier understands quote-based purchasing for professional healthcare customers rather than retail-style order handling. Coronary intervention procedures often require account-specific quoting, volume discussion, and coordinated sourcing around preferred manufacturers.
For international customers, export capability is part of the product offer. A broad device portfolio is less valuable if cross-border fulfillment, documentation, and communication are inconsistent. This is one reason many professional buyers prefer working with a wholesale source that already supports global branded-device procurement through a single inquiry flow, such as IMTMedicalDevices.com.
A more realistic way to think about coronary intervention procedures
The most useful procurement view is simple: coronary intervention procedures are not one product category. They are a repeatable but variable device ecosystem where the outcome for the buyer is case readiness, not just purchase completion.
That changes how inventory should be planned. Instead of asking whether a facility has coronary wires, balloons, and stents in general, the better question is whether it has the right branded combinations available for the cases it actually treats, with enough continuity to support physician preference and enough flexibility to handle the cases that become more complex than expected.
For procurement teams, that is usually where value shows up - not in the broad promise of supply, but in getting the exact devices needed for the next case, the next shipment, and the next quote without unnecessary friction.