How Hospitals Source Guidewires
A guidewire shortage rarely starts with the wire itself. It usually starts when a cath lab needs a specific tip load, coating, diameter, or brand preference for a case mix that cannot tolerate substitution. That is why how hospitals source guidewires is less about ordering a generic category and more about securing exact branded SKUs with dependable availability, regulatory alignment, and traceable supply.
How hospitals source guidewires in practice
Most hospitals do not buy guidewires as a broad commodity line. They buy against procedure demand, physician preference, existing contracts, and approved product lists. In interventional cardiology, peripheral intervention, interventional radiology, and neurovascular work, the required wire characteristics can be highly specific. A purchasing team may be asked for a hydrophilic wire from one manufacturer for peripheral access, a workhorse coronary wire from another brand for routine PCI, and a specialty wire with precise torque response for more complex anatomy.
In practice, sourcing starts with a defined need signal. That signal may come from usage history, upcoming cases, par levels in the cath lab, or a request from clinicians who need continuity with a known platform. From there, procurement teams validate manufacturer, product family, dimensions, packaging configuration, and approval status before requesting quotes from contracted suppliers or specialized wholesale sources.
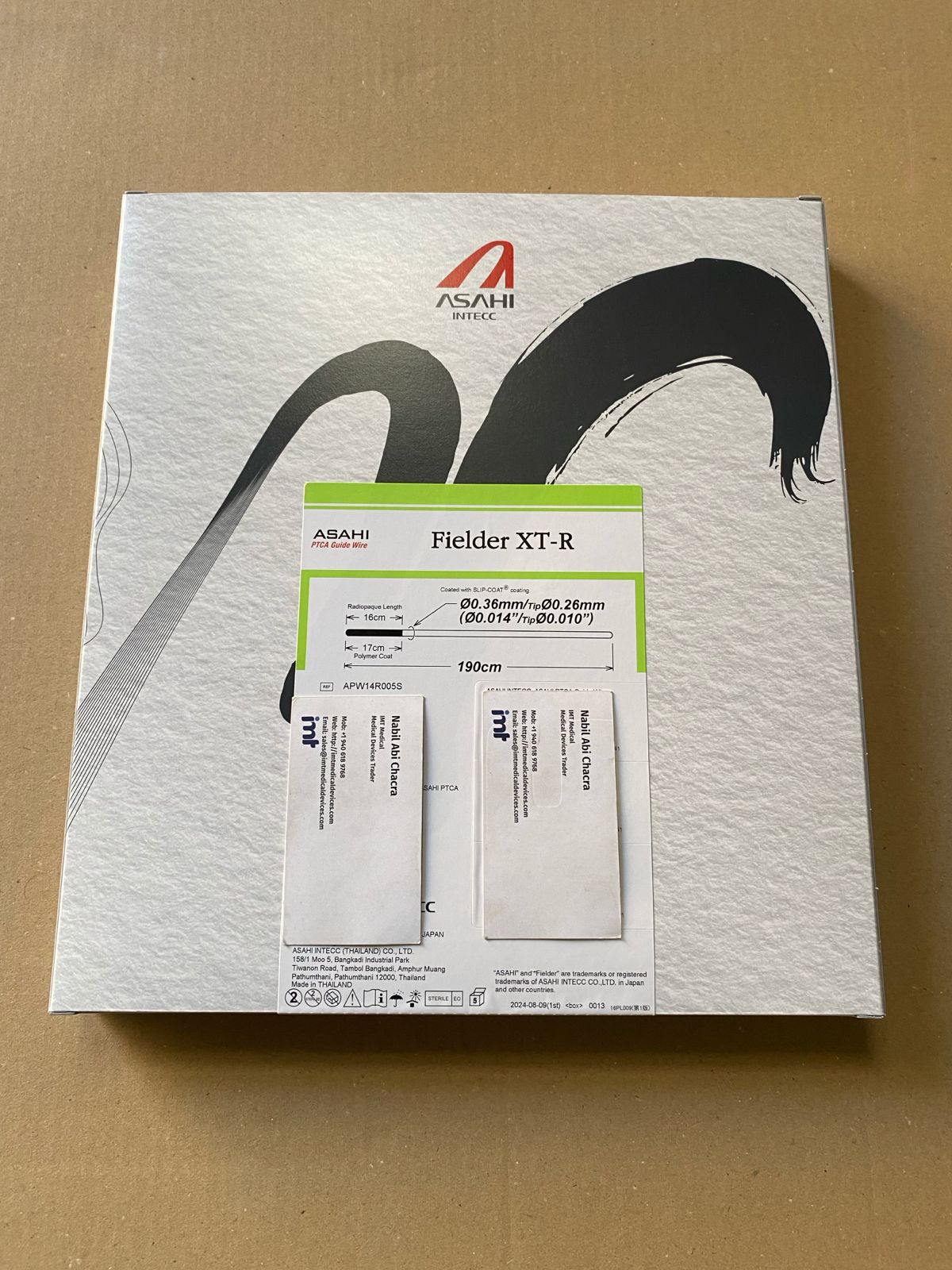
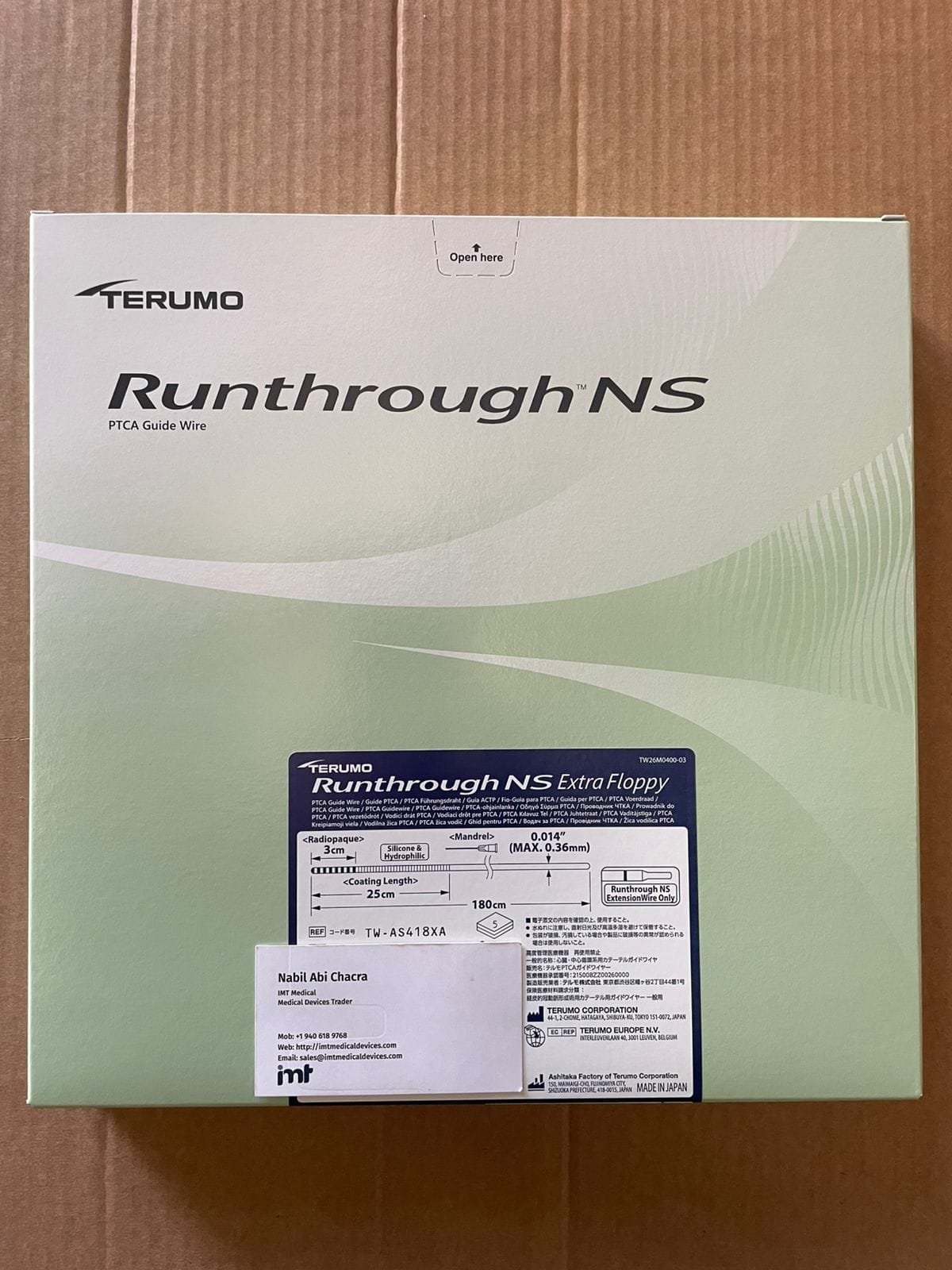
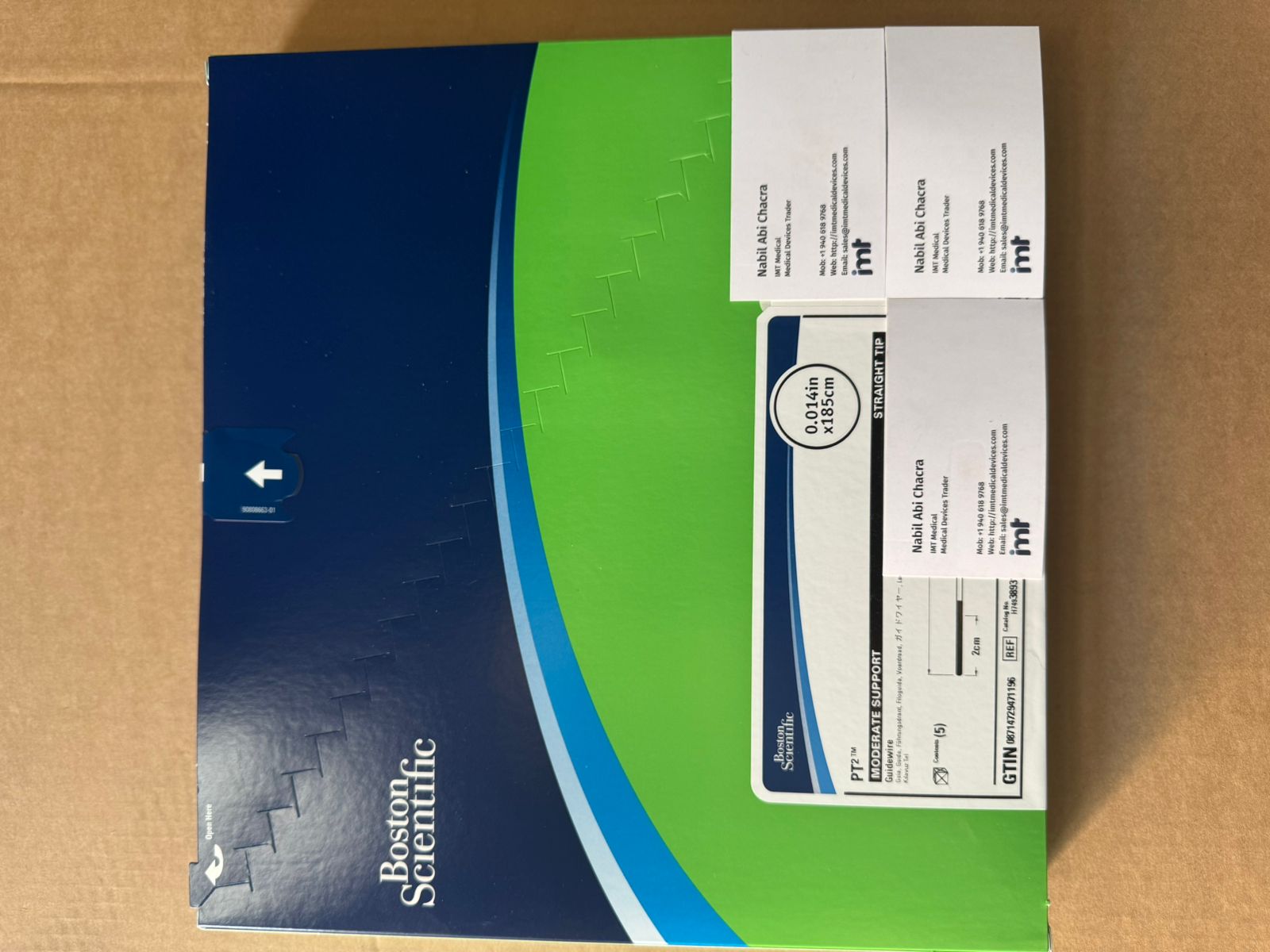
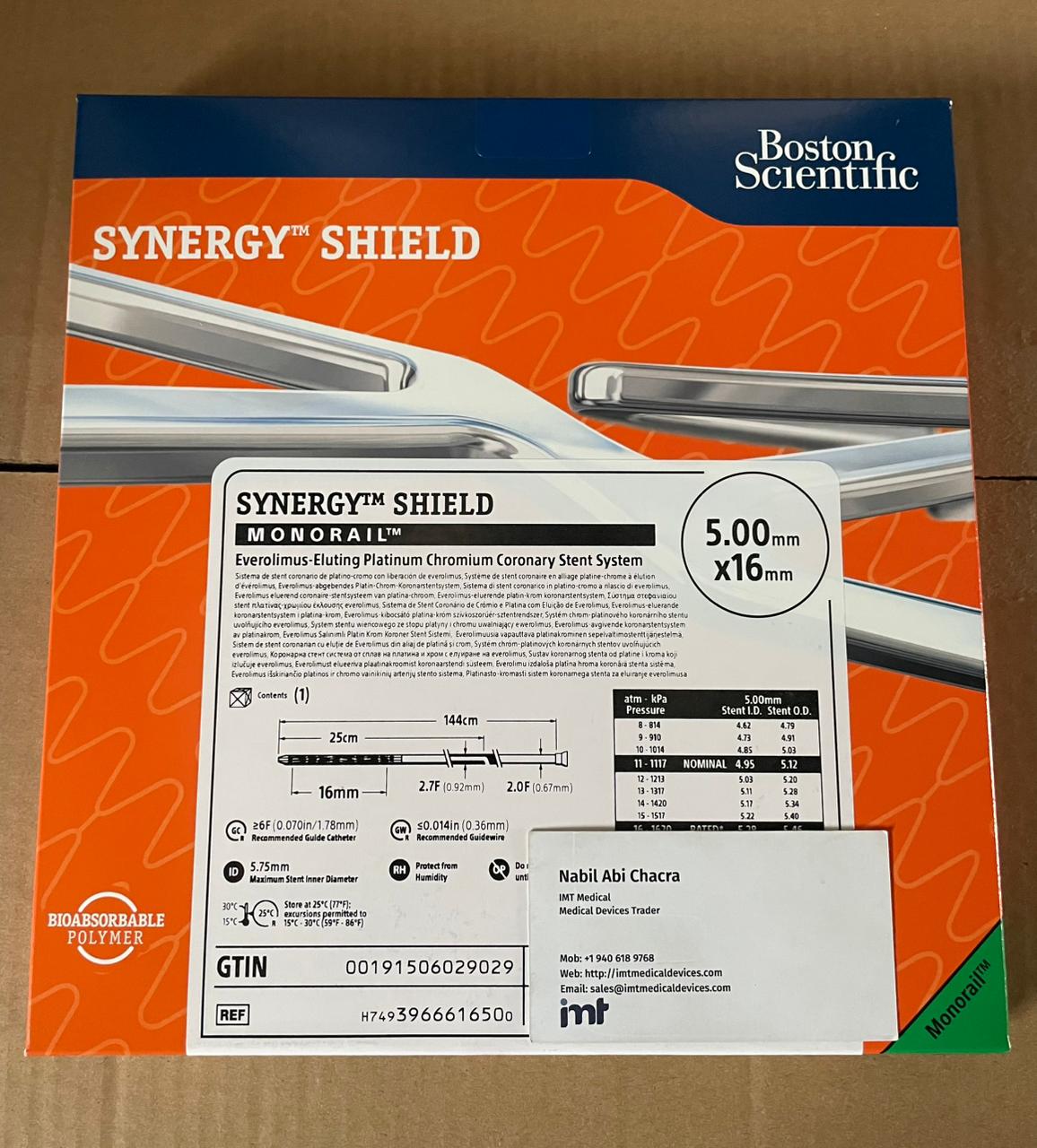
This is also why branded device sourcing remains central. When clinicians are trained on Terumo, Asahi, Boston Scientific, Abbott, Medtronic, or Cordis platforms, the hospital is not simply choosing a guidewire category. It is choosing a familiar device profile with known handling characteristics and clinical acceptance inside the department.
The main factors procurement teams evaluate
The first factor is exact product identification. Guidewires are sourced by manufacturer name, product line, size, coating, tip design, shaft construction, and SKU. A request that lacks one of these details often slows the process. For procurement, SKU accuracy matters because near-equivalent alternatives are not always clinically interchangeable, even when they appear similar on paper.
The second factor is approval and market suitability. Hospitals need products aligned with their regulatory and institutional requirements. That can mean checking labeling, country-specific import documentation, and whether the product is acceptable under local policy. For international buyers, this becomes more complex because the same branded line may have different packaging configurations or market availability depending on destination.
The third factor is supply continuity. A lower quoted price has limited value if the supplier cannot support repeat orders. Guidewires are tied to ongoing procedural volumes, not one-time purchasing events. Procurement teams usually prefer suppliers that can support recurring demand, provide realistic lead times, and confirm stock on high-turn SKUs.
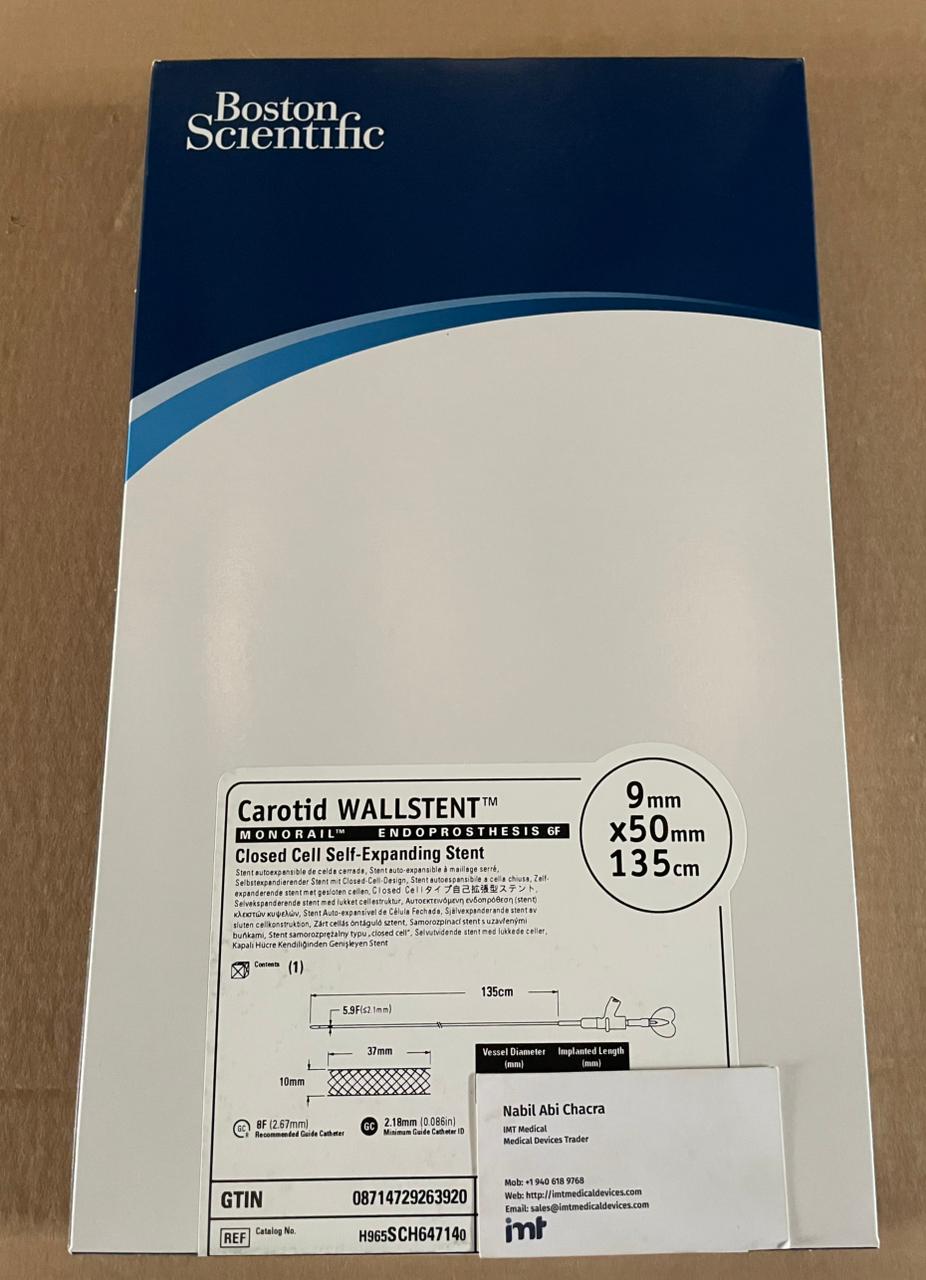
The fourth factor is sourcing efficiency across multiple categories. Hospitals and distributors often prefer suppliers that can consolidate coronary, peripheral, neurovascular, and related device lines into one quote process. This reduces administrative friction and makes replenishment easier, especially when multiple physician teams are drawing from separate approved brands.
Why physician preference shapes sourcing decisions
Guidewire procurement is one of the clearest examples of clinical preference affecting purchasing. A physician may trust a specific wire for support, crossing behavior, or tactile feedback in a given anatomy. In routine cases, substitution may be possible if the lab has already validated comparable products. In more specialized procedures, substitution can create resistance because the perceived procedural risk rises when device feel changes.
For procurement teams, this means sourcing is partly technical and partly operational. The technical side involves product specifications. The operational side involves maintaining alignment between what clinicians want to use and what the hospital can source consistently under budget and policy constraints.
There is always a trade-off here. Standardization can improve pricing and inventory control, but over-standardization can create problems when a case requires a less common wire. The most effective sourcing programs usually maintain a core set of high-usage guidewires and a narrower range of specialty options tied to documented procedural need.
Contracted channels vs specialized wholesale sourcing
Hospitals often begin with existing purchasing contracts or local authorized channels. That is the straightforward path when the required guidewire is stocked, approved, and available on acceptable terms. But hospitals also encounter gaps. A contracted supplier may be out of stock, may not support a needed international shipment, or may not carry the full mix of brands required across service lines.
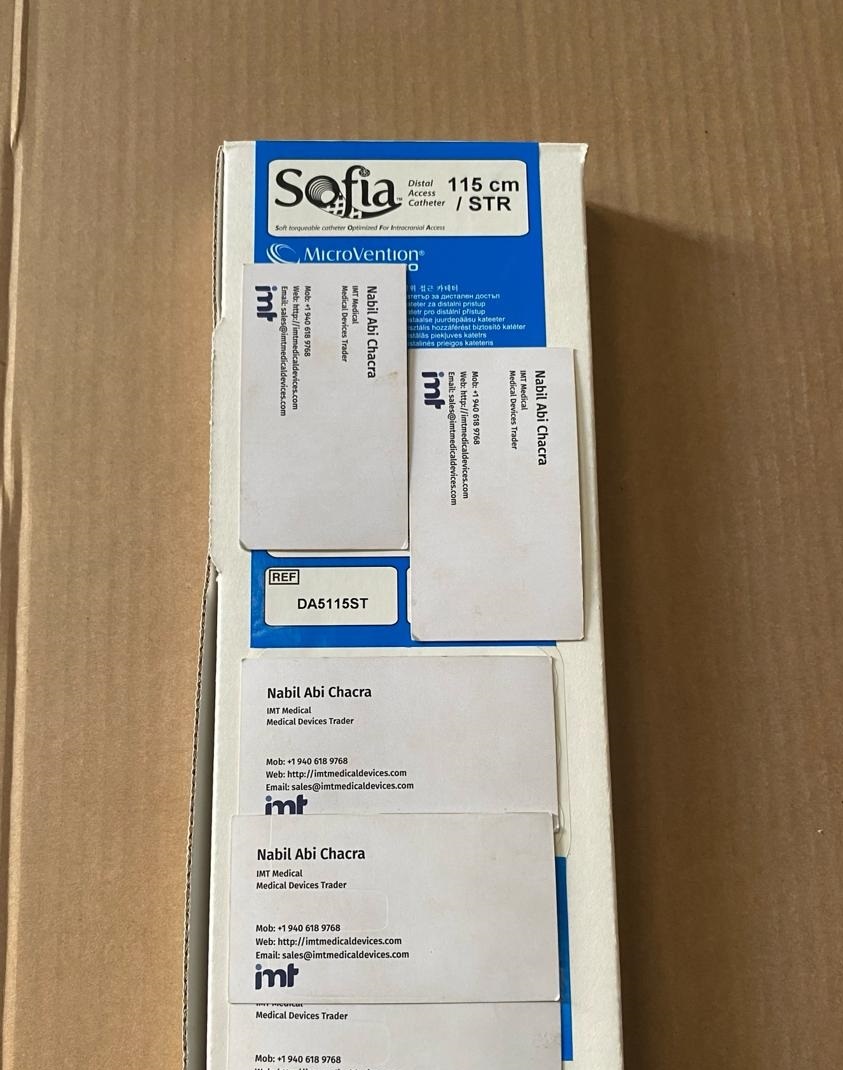
This is where specialized wholesale sourcing becomes relevant. A supplier with access to multiple globally recognized manufacturers can help buyers consolidate demand across brands and intervention types. For procurement departments managing cardiology, IR, peripheral, neurovascular, and laboratory purchasing, this matters because the buying workflow becomes faster when fewer vendor touchpoints are involved.
That said, hospitals do not shift sourcing lightly. They evaluate whether the supplier understands branded medical device procurement, can quote accurately by SKU, can provide export support where needed, and can maintain a professional standard of documentation. For international buyers, export capability is not an extra feature. It is part of the sourcing requirement.
How hospitals source guidewires when availability is tight
When availability tightens, hospitals typically move from routine replenishment to exception-based sourcing. Buyers review acceptable alternatives, contact secondary suppliers, and prioritize products based on procedural urgency. The challenge is that a shortage in one guidewire line can ripple into scheduling decisions if the substitute is not clinically accepted by the lab.
This is why supplier responsiveness matters as much as catalog breadth. Procurement teams need direct answers on stock status, lot traceability, lead time, and brand availability. Vague availability language slows decisions. Clear quote-based communication helps buyers determine whether to wait, substitute, or split the order across sources.
In these periods, buyers also pay closer attention to authenticity and chain of custody. With high-demand branded devices, a hospital needs confidence that products are genuine, properly handled, and documented for professional use. Price pressure tends to increase during shortages, but hospitals cannot treat guidewires as a gray-market category.
The role of international procurement
Not every hospital sources only from domestic channels. Many healthcare buyers, distributors, and medical supply organizations work across borders because branded device availability is uneven by market. International sourcing can help secure specific manufacturers, fill portfolio gaps, or support buyers in regions where local access is limited.
This approach has advantages, but it also requires discipline. Buyers need clarity on export documentation, destination requirements, shipping terms, and whether the supplier regularly handles international fulfillment. The best international sourcing relationships are built on exact product matching and realistic logistics, not broad promises.
For organizations buying in volume, an international wholesale partner can also reduce fragmentation. Instead of contacting separate sources for coronary wires, peripheral devices, closure products, and neurovascular consumables, procurement can centralize quote requests through one channel. For many professional buyers, that administrative efficiency is as valuable as the unit economics.
Common sourcing mistakes hospitals try to avoid
One common mistake is sourcing by generic description rather than exact reference. A request for a coronary guidewire without the preferred brand, diameter, length, coating type, and part number usually leads to back-and-forth that delays fulfillment.
Another mistake is treating one-time availability as a sourcing solution. If a supplier can deliver a needed wire once but cannot support future demand, the hospital may solve the immediate problem while creating a longer-term continuity issue.
A third mistake is separating procurement from end-user input. If buyers source based only on price and broad category match, they may end up with products that clinicians resist using. That often creates urgent reordering and duplicate inventory costs.
What strong guidewire sourcing looks like
Strong sourcing is usually quiet. The lab has the right wires on hand, physicians are not escalating last-minute substitutions, and procurement has clear visibility into approved brands, reorder patterns, and backup sources. It is not built on a single vendor claim. It is built on disciplined SKU management, credible supply relationships, and a sourcing process that reflects actual procedural demand.
For many buyers, the most practical model is a combination of standard contracted purchasing and qualified wholesale support for branded device access, portfolio breadth, and international fulfillment. A supplier such as IMT Medical Devices fits this model when a buyer needs recognized manufacturers, exact product identification, and quote-based sourcing across multiple intervention categories.
Hospitals that source guidewires well tend to ask simple but demanding questions: Is this the exact SKU? Is it approved for our market? Can the supplier support repeat demand? Can they ship where we need it? Those questions keep procurement aligned with clinical use, and that is usually where better purchasing decisions start.